A pressure ulcer on the foot can start as a small red spot and quickly become a serious wound that threatens your mobility, and in some cases, your limb. Whether it developed from prolonged bed rest, a poorly fitting shoe, or reduced sensation caused by diabetes, finding the right pressure ulcer on foot treatment matters more than most people realize. Left unaddressed, even a shallow ulcer can deepen into muscle and bone, leading to infection, hospitalization, or amputation.
The good news: most pressure ulcers on the foot can heal when you follow a structured treatment plan that combines proper wound care, consistent offloading, and close monitoring. But knowing what to do, and when to escalate care, is the difference between a wound that closes in weeks and one that lingers for months. That’s exactly what this article breaks down, step by step, so you can take informed action right away.
At Achilles Foot and Ankle Center, our team treats pressure ulcers and chronic wounds across thirteen locations in Central Virginia, using advanced wound care and limb salvage protocols in our state-of-the-art facilities. We see firsthand how early, expert intervention changes outcomes. Below, you’ll find the treatment steps, dressing options, offloading strategies, and warning signs that should prompt you to call a podiatrist, all drawn from the kind of care we provide every day.
Why pressure ulcers on feet need fast care
The foot sits at the bottom of your circulatory system, which means blood already works harder to reach it and return to your heart. When sustained pressure cuts off that flow to a small patch of skin, tissue begins breaking down faster than most people expect. A wound that looks minor on the surface can already involve damage to deeper layers, and the foot’s anatomy, with tendons, joints, and bones sitting close beneath the skin, means infection can spread rapidly once it finds an entry point.
The foot heals more slowly than other body parts
Your feet carry your full body weight throughout the day, creating constant mechanical stress on any wound that is trying to close. Reduced circulation, which is common in people with diabetes, peripheral artery disease, or heart conditions, means oxygen and nutrients reach the wound site more slowly. This slows every phase of healing: inflammation, tissue formation, and skin closure all take longer than they would on other parts of the body. Without consistent pressure relief and circulatory support, even a wound you clean and dress correctly can stall or worsen within days.
People with peripheral neuropathy, a form of nerve damage that reduces or eliminates foot sensation, face an additional complication. They often cannot feel the wound at all, so they continue putting weight on it without knowing the damage they are causing. By the time a wound becomes visible or starts affecting daily movement, it has frequently already progressed past the earliest and most treatable stages, making intervention both more urgent and more complex.
Starting pressure ulcer on foot treatment at Stage 1 or Stage 2 gives you the best chance of healing without surgical intervention.
How infection takes hold quickly in foot wounds
The foot contacts more surfaces and more bacteria throughout the day than almost any other part of the body, making an open wound there a direct entry point for serious infection. Bacteria such as Staphylococcus aureus thrive in moist wound environments, and a neglected pressure ulcer can develop a biofilm, a protective coating that allows bacteria to resist standard cleaning. Once infection reaches bone tissue, a condition called osteomyelitis, treatment typically requires intravenous antibiotics and, in many cases, surgical removal of the infected bone itself.
Systemic complications from foot infections are not rare. Sepsis, a dangerous immune response to infection spreading through the bloodstream, can develop within days in someone with compromised immunity or poor circulation. For people with diabetes specifically, wound infection is one of the leading causes of lower-limb amputation in the United States, according to the Centers for Disease Control and Prevention. That risk alone explains why waiting to address a foot pressure ulcer, even one that appears manageable at home, is rarely a safe choice.
How to treat a pressure ulcer on your foot
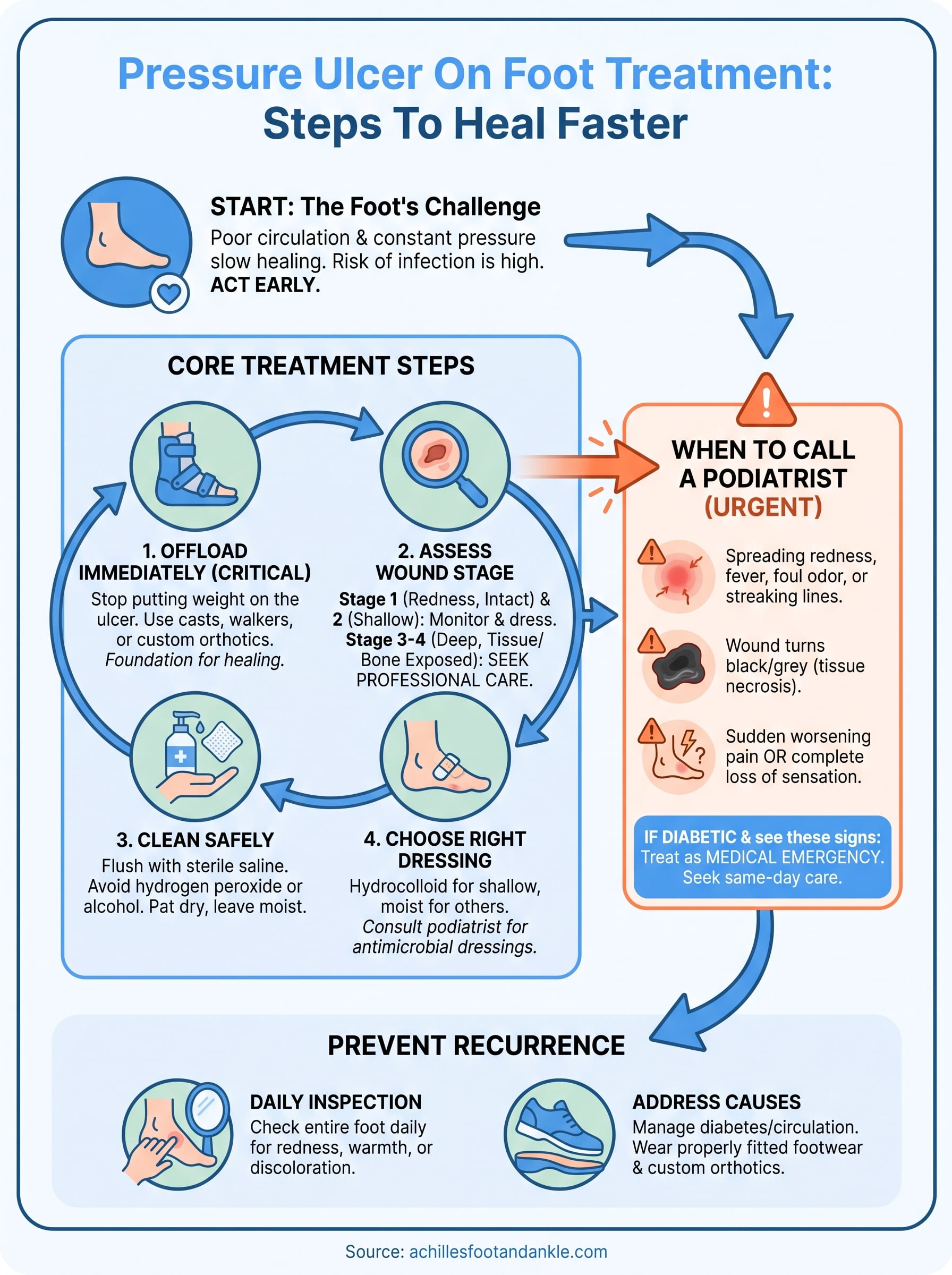
Effective pressure ulcer on foot treatment follows a clear sequence: remove pressure, assess the wound, clean it, apply the right dressing, and monitor for infection. Skipping steps or doing them out of order is one of the most common reasons foot ulcers stall instead of heal. Before applying anything to the wound, address the two fundamentals that determine whether any other treatment will actually work.
Remove pressure from the wound immediately
The single most important action you can take is to stop putting weight on the ulcer. Continued pressure blocks blood flow to the wound site and shuts down healing regardless of what dressing or ointment you apply. Offloading means shifting pressure away from the damaged tissue, and your options range from complete bed rest to specialized footwear. A total contact cast distributes weight evenly across the entire foot and is one of the most effective offloading tools for plantar ulcers. Removable cast walkers and therapeutic shoes can work for less severe wounds, but only if you wear them consistently.
Offloading is not optional in pressure ulcer treatment. It is the foundation every other step depends on.
A custom orthotic or padding inside a well-fitting shoe can redirect pressure away from a vulnerable spot if your wound is early-stage and not yet open. Talk to a podiatrist before using any padding on an open wound, since improper application can trap moisture and worsen infection risk.
Assess the wound stage before choosing a treatment
Stage 1 and Stage 2 ulcers, where skin is intact or shallowly broken, often respond to conservative care combined with professional monitoring. Stage 3 and Stage 4 ulcers, which extend into fat, muscle, or bone, require professional wound care and frequently need surgery. Use this as a quick reference:

- Stage 1: Skin intact, persistent redness. Offload and monitor closely.
- Stage 2: Shallow open wound or blister. Dress the wound and see a podiatrist.
- Stage 3-4: Tissue or bone exposed. Seek professional care immediately.
How to clean and dress the wound safely
Cleaning and dressing your wound correctly is where many home treatment attempts break down. Using the wrong solution, touching the wound bed with dry gauze, or changing dressings too infrequently can introduce bacteria and damage fragile tissue that is just starting to rebuild. Proper wound hygiene is as important as offloading in any pressure ulcer on foot treatment plan, and the steps below apply every time you change the dressing.
Clean the wound before every dressing change
Before you touch the wound, wash your hands thoroughly with soap and water and put on clean disposable gloves. Rinse the ulcer with sterile saline solution, which you can find at most pharmacies, by gently flushing the wound rather than rubbing it. Rubbing pulls away newly forming tissue and slows healing. Avoid using hydrogen peroxide, iodine, or alcohol directly on the wound bed; these products kill bacteria but also destroy the healthy cells your body is producing to close the wound.
Saline is the safest and most effective solution for routine pressure ulcer wound cleaning at home.
After rinsing, pat the surrounding skin dry with a clean cloth or gauze pad. Leave the wound bed moist, not wet, before applying your dressing. Moisture at the wound surface supports tissue growth, while excess fluid sitting on the wound encourages bacterial overgrowth.
Choose the right dressing for the wound stage
Your wound stage determines which dressing performs best. Hydrocolloid dressings work well for Stage 1 and shallow Stage 2 ulcers because they maintain a moist environment and protect the wound from friction. Foam dressings absorb more drainage and suit wounds producing moderate fluid output. Antimicrobial dressings containing silver are appropriate when you see early signs of infection, such as increased redness, warmth, or odor, but a podiatrist should confirm that choice before you apply one. Change dressings according to the product instructions, typically every one to three days, or sooner if the dressing becomes saturated.
When you need a podiatrist or urgent care
Home care has a clear limit, and recognizing that limit early is part of any effective pressure ulcer on foot treatment plan. If your wound is not showing signs of improvement within two weeks of consistent care, or if it is deepening rather than shrinking, professional wound assessment is no longer optional. A podiatrist can identify complications that are invisible to the untrained eye and access treatments that simply are not available over the counter.
Signs that require same-day or urgent attention
Some changes in a foot ulcer signal a situation that cannot wait for a scheduled appointment. Spreading redness, streaking lines extending from the wound, fever, or a foul odor all indicate that infection has moved beyond the wound surface and requires immediate evaluation. If you notice the wound bed turning black or grey, tissue necrosis, which is dead tissue, is present and debridement by a clinician is necessary before healing can begin at all.

If you have diabetes and notice any of these signs, treat the situation as a medical emergency and seek care the same day.
Pain that suddenly worsens, or the opposite, a complete loss of sensation around the wound, also warrants urgent evaluation, since both changes suggest your circulation or nerve function is compromised in a way that dramatically raises your amputation risk.
What a podiatrist will do that you cannot do at home
A podiatrist brings tools and clinical judgment that change treatment outcomes. They can debride necrotic tissue safely, removing dead material that blocks wound closure without damaging surrounding healthy cells. They can also order imaging to check whether infection has reached the bone, prescribe targeted antibiotics, and fit you with properly calibrated offloading devices based on your specific foot structure and wound location. In cases where the wound has progressed to Stage 3 or Stage 4, surgical intervention such as skin grafting or reconstructive surgery may be the only path to closure, and a podiatrist is the specialist equipped to make and execute that call.
How to prevent pressure ulcers from coming back
Healing a pressure ulcer is only half the work. Without changing the conditions that caused it, the same wound can return within weeks, often in the same spot or somewhere new. Preventing recurrence is a direct extension of any pressure ulcer on foot treatment plan, and it requires consistent daily habits rather than occasional attention.
Inspect your feet daily and manage pressure points
You should check the entire surface of both feet every single day, including the heel, ball, and between the toes. Use a mirror or ask someone to help if you have limited mobility or cannot see the underside of your feet clearly. Look for redness, warmth, blisters, or any area that appears discolored, since catching these early signs before the skin breaks gives you the best chance of stopping a full ulcer from forming.
Daily foot inspection takes less than two minutes and is one of the most effective tools you have for preventing recurrence.
Custom orthotics and properly fitted footwear redistribute pressure away from vulnerable areas and reduce the mechanical forces that cause tissue damage in the first place. Work with your podiatrist to identify your specific pressure points and get footwear or insoles designed around your actual foot shape.
Address the underlying causes that make you vulnerable
If diabetes, peripheral artery disease, or neuropathy contributed to your first ulcer, managing those conditions directly reduces your recurrence risk. Keeping blood sugar controlled, following up with your vascular team if circulation is poor, and attending regular podiatry appointments all work together to keep your feet in better health over time.
Nutrition also plays a measurable role in skin integrity and tissue resilience. Adequate protein, vitamin C, and zinc support your skin’s ability to withstand pressure. Talk to your doctor about whether your current diet meets those needs, especially if you have a condition that affects how your body absorbs nutrients.
What to do today
You now have a complete picture of pressure ulcer on foot treatment, from offloading and wound cleaning to knowing when to call a specialist. The most important thing you can do right now is act on what you have read rather than wait to see if the wound improves on its own. Start inspecting your foot today, remove pressure from any affected area, and gather the supplies you need to clean and dress the wound correctly.
If your wound is already open, deepening, or showing signs of infection, or if you have diabetes or poor circulation, do not delay professional evaluation. The earlier a podiatrist assesses your ulcer, the more treatment options you have and the lower your risk of serious complications. Contact our team at Achilles Foot and Ankle Center and schedule a same-day appointment so we can assess your wound and build a plan that gets you healing faster.