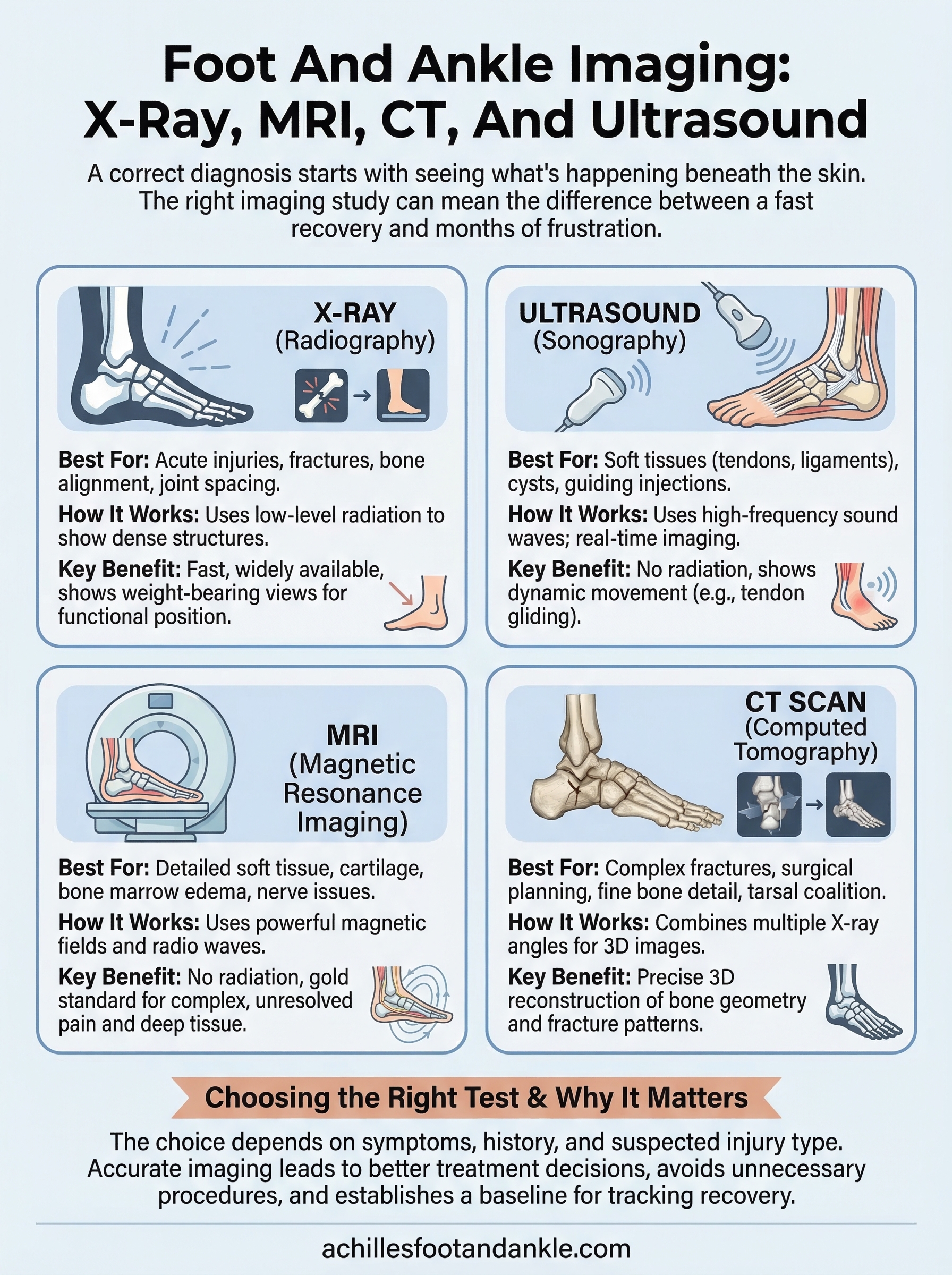
A correct diagnosis starts with seeing what’s happening beneath the skin. Foot and ankle imaging gives your doctor a direct look at bones, soft tissues, joints, and ligaments, information that a physical exam alone can’t always provide. Whether you’re dealing with a stress fracture that won’t heal, chronic heel pain, or an ankle injury from the basketball court, the right imaging study can mean the difference between a fast recovery and months of frustration.
At Achilles Foot and Ankle Center, our specialists across Central Virginia use advanced diagnostic imaging technology, including digital X-ray, MRI, CT, and ultrasound, every day to pinpoint the source of foot and ankle problems. We rely on these tools not just to confirm what we suspect, but to rule out what we don’t, giving each patient a clear and accurate picture before recommending any treatment plan.
This article breaks down the four primary imaging modalities used in foot and ankle care: what each one shows, when it’s ordered, and why your podiatrist might choose one over another. You’ll learn how X-rays differ from MRIs, when a CT scan adds value, and where ultrasound fits into the diagnostic process. By the end, you’ll have a practical understanding of these tools so you can walk into your next appointment informed and confident about what comes next.
Why foot and ankle imaging matters
The foot and ankle work together as a single mechanical unit that absorbs and distributes millions of pounds of force over a normal week of activity. With 26 bones, 33 joints, and more than 100 tendons, ligaments, and muscles packed into a compact area, even a minor structural problem can send pain radiating through your entire lower limb. Imaging gives your clinician a precise look at that complexity without guessing.
Accurate imaging is not optional for complex foot and ankle conditions; it is the foundation of an effective treatment plan.
The structural complexity underneath your feet
Your foot and ankle contain more bones relative to their size than almost any other region of the body. The 26 bones in your foot include the heel bone (calcaneus), the talus that connects your foot to your lower leg, and five long metatarsal bones that support the forefoot. Each joint between those bones is lined with cartilage and stabilized by ligaments, and damage to any single structure can alter how every neighboring structure functions over time.
This density of anatomy explains why two patients can describe nearly identical symptoms and end up with completely different diagnoses. You might feel sharp pain along the outside of your ankle from a ligament tear, a peroneal tendon injury, or a stress fracture of the fifth metatarsal. Foot and ankle imaging is what separates those possibilities and points your doctor toward the right course of action from the first appointment rather than several visits later.
What imaging reveals that physical exams cannot
A skilled clinician can learn a great deal from pressing on your foot, watching you walk, and testing your range of motion. Physical examination has clear limits, though. Soft tissue injuries deep inside the ankle, early stress fractures in the metatarsals, and subtle changes in bone marrow are invisible to even the most experienced hands. These conditions require technology that sees through skin and muscle to give your doctor a reliable answer.
Delayed diagnosis is one of the most common reasons a straightforward injury turns into a chronic problem. A stress fracture that resembles a sprain on examination can become a complete break if you keep walking on it for weeks without proper imaging. Tendon degeneration that presents as general heel pain can silently progress to a full rupture if the underlying tissue damage goes undetected. Early imaging catches these conditions while they are still manageable and far easier to treat.
How imaging supports better treatment decisions
Ordering the right scan early in your care also protects you from unnecessary procedures. If your podiatrist confirms on ultrasound that your Achilles tendon has mild tendinopathy with no tearing, you skip surgery entirely and move directly into physical therapy. If an MRI shows significant cartilage loss in the ankle joint, your treatment team can plan a targeted intervention rather than cycling through months of conservative care that won’t address the underlying problem.
Imaging results also create a measurable baseline for tracking your progress. When your doctor takes a weight-bearing X-ray at your first appointment and then another six weeks into treatment, the side-by-side comparison shows whether the bone is healing, the deformity is correcting, or the selected approach is working as expected. That kind of objective, visual data gives both you and your provider the confidence to stay on course or change direction when needed.
How clinicians choose the right imaging test
No imaging test covers every situation equally well. Your podiatrist follows a structured decision-making process that weighs your symptoms, medical history, and the likely diagnosis before selecting a scan. That process helps avoid unnecessary tests and gets you to an accurate answer as efficiently as possible.
Starting with your symptoms and history
Before ordering any scan, your clinician reviews the full picture of your complaint. How long you’ve had the pain, whether it came on suddenly or built up gradually, and which activities make it worse all shape the decision. A patient who twisted their ankle stepping off a curb yesterday points toward a different initial test than a patient who has had dull forefoot aching for three months during morning runs.
Your previous imaging studies, surgeries, and existing medical conditions also matter. If you’ve had metal hardware placed from a prior ankle surgery, that rules out standard MRI and shifts your doctor toward CT or ultrasound instead. If you have diabetes and a non-healing wound, bone scan or MRI of the midfoot moves much higher on the list because identifying bone infection early is critical for limb preservation.
Choosing the right imaging test upfront avoids the delay of starting with the wrong one and repeating the entire process later.
Matching the scan to the injury type
Once your clinician understands the likely problem, the structural nature of the injury drives the final choice. Bone problems generally call for X-ray or CT. Soft tissue injuries, including tendon tears, ligament damage, and cartilage loss, typically require ultrasound or MRI to visualize properly. Foot and ankle imaging decisions also account for the anatomical layer involved: surface-level soft tissue lesions are often faster and more cost-effective to assess with ultrasound, while deep joint and bone marrow changes need the resolution that MRI provides.
Practical factors play a role too. Cost, insurance coverage, and equipment availability at your specific clinic location can influence which test comes first, especially when two options would provide similar diagnostic value. In straightforward cases, your podiatrist may start with X-ray and only advance to MRI or CT if those results don’t fully explain your symptoms. This stepwise approach keeps your care efficient without sacrificing the accuracy you need to move forward with confidence.
X-ray for foot and ankle problems
X-ray is the first tool most clinicians reach for when you walk in with foot or ankle pain, and for good reason. It’s fast, widely available, and delivers immediately useful information about bone alignment, joint spacing, and obvious fractures. For the majority of acute injuries and structural concerns, an X-ray gives your podiatrist enough to either confirm a diagnosis or identify what needs a closer look.
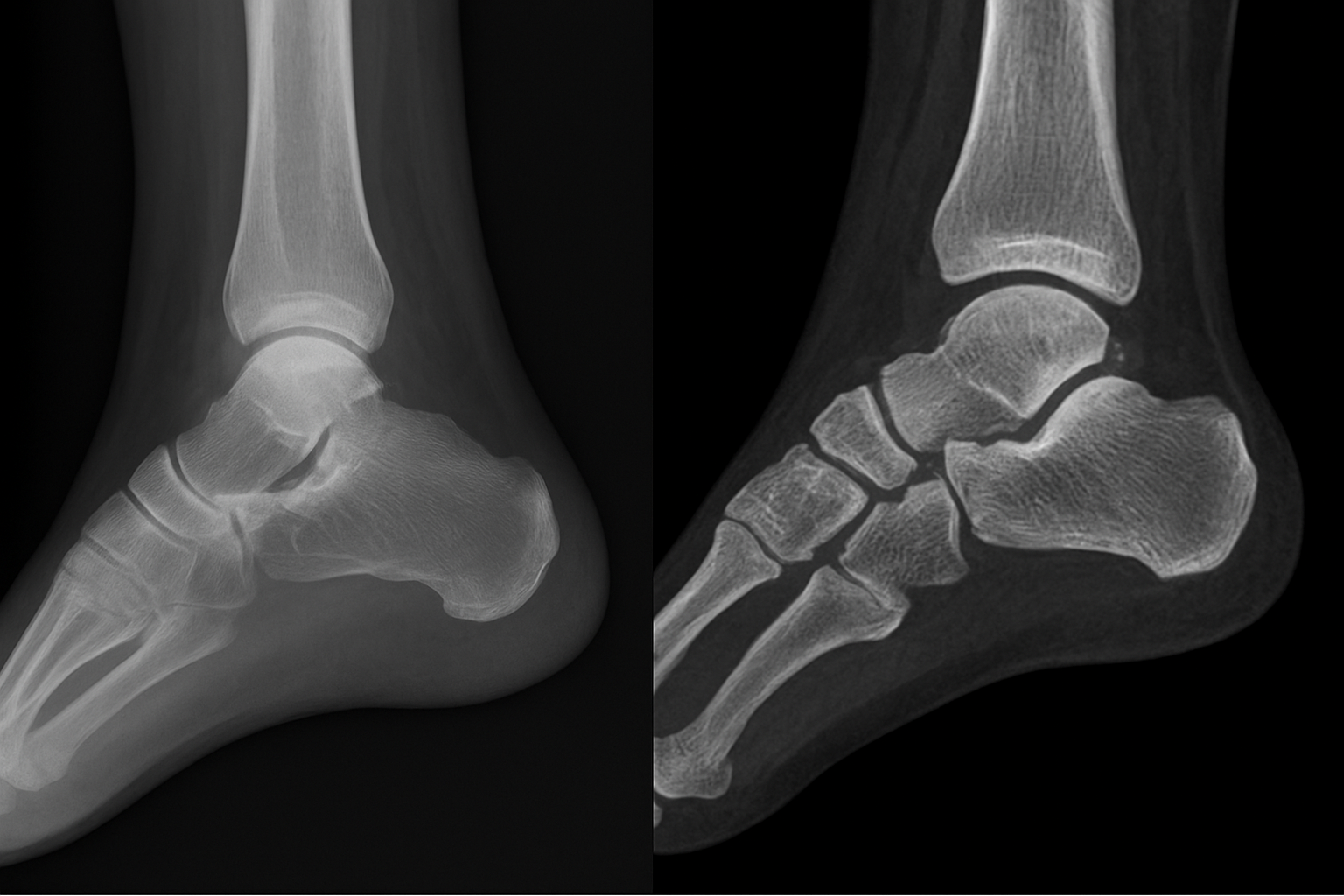
What X-rays show and when doctors order them
X-ray uses low-level radiation to produce images of dense structures, primarily bone, with excellent clarity. Your doctor can quickly identify fractures, dislocations, arthritis-related joint narrowing, bone spurs, and deformities like bunions or flatfoot collapse. Foot and ankle imaging that starts with X-ray also helps detect foreign bodies such as glass or metal fragments that may have entered the tissue after a puncture wound.
Your podiatrist will typically order X-rays first when you report a sudden injury, persistent localized bone pain, or a visible deformity. They’re also routine before any surgical planning because they provide a full structural overview of how your bones align and how much space remains between joints. In many cases, a clear X-ray finding is all that’s needed to move forward with a treatment plan without advancing to more complex or expensive studies.
X-ray remains the most practical starting point in foot and ankle imaging because it answers the most common clinical questions quickly and at low cost.
Weight-bearing X-rays and why positioning matters
One detail that separates foot and ankle X-rays from imaging in other body parts is the importance of weight-bearing views. When you stand on your foot and put your full body weight through it, the bones shift into the positions they actually occupy during your daily life. A non-weight-bearing X-ray taken while you’re lying on a table can miss subtle flatfoot deformity, Lisfranc joint instability, or forefoot splay that only become visible under load.

Your technician may take X-rays in multiple positions during a single visit: from the side, from above, and at an angle called the oblique view. Each projection highlights different structures and eliminates the overlap that can hide a small fracture or joint change in a single-angle image. When your clinician reviews all three views together, they build a much more complete picture of your foot’s structure than any single image could provide on its own.
Ultrasound for tendons, ligaments, and soft tissue
Ultrasound uses high-frequency sound waves to produce real-time images of soft tissue structures that X-ray simply cannot see. When your podiatrist suspects a tendon tear, ligament injury, or fluid-filled cyst near a joint, ultrasound is often the fastest and most practical next step. It requires no radiation, no large machine, and no lengthy wait for imaging availability at a separate facility, which makes it a valuable tool during the same clinic visit where you first describe your pain.
What ultrasound reveals in real time
Your clinician can use ultrasound to examine the Achilles tendon, peroneal tendons, plantar fascia, and ankle ligaments with high resolution and immediate feedback. The imaging shows the internal structure of each tendon, including areas of degeneration, partial tearing, and abnormal thickening that indicate chronic overload. Fluid accumulation around a tendon sheath or within a bursa also appears clearly on ultrasound, helping your podiatrist distinguish between mechanical irritation and inflammatory conditions that require different treatment approaches.

One major advantage of ultrasound in foot and ankle imaging is dynamic assessment. Your technician can move your ankle or toe while imaging, watching how tendons glide through their sheaths in real time. A tendon that snaps or subluxes out of position during movement is visible on ultrasound in a way that a static MRI scan simply cannot capture. This live view adds a layer of diagnostic accuracy that no other imaging modality offers for soft tissue problems.
Dynamic ultrasound is the only imaging tool that shows how tendons and ligaments actually behave during movement, not just how they appear at rest.
When ultrasound is the right choice
Your doctor will typically reach for ultrasound when your symptoms point strongly toward a specific tendon or ligament as the source of pain, particularly along the back, inside, or outside of the ankle. It’s also the preferred modality for guiding injections, whether your podiatrist is delivering a corticosteroid into a tendon sheath or aspirating fluid from a ganglion cyst. Ultrasound-guided procedures improve accuracy significantly compared to landmark-based injections, reducing the risk of missing the target structure entirely.
Ultrasound does have limits. Deep bone marrow changes, cartilage surfaces inside joints, and structures obscured by bone fall outside what sound waves can image reliably. When your soft tissue symptoms are complex or don’t match what ultrasound reveals, your clinician will advance to MRI for a more comprehensive view of the entire joint.
MRI for detailed soft tissue and bone marrow changes
Magnetic resonance imaging uses powerful magnetic fields and radio waves to produce detailed cross-sectional images of every tissue layer in your foot and ankle. Unlike X-ray or CT, MRI does not use radiation. It excels at showing cartilage surfaces, bone marrow, tendons, ligaments, and nerves with a level of detail that no other imaging modality can match, making it the gold standard for complex or unresolved foot and ankle complaints.
What MRI shows that other scans miss
MRI’s greatest strength in foot and ankle imaging is its ability to detect bone marrow edema, which is the fluid accumulation inside bone that appears before a stress fracture becomes visible on X-ray. When you have deep, aching pain in your midfoot or heel that doesn’t improve with rest, bone marrow changes on MRI can identify the problem days or even weeks earlier than any other test available. That early detection matters because it changes your treatment plan immediately, before the injury has the chance to worsen.

Beyond bone marrow, MRI captures cartilage damage inside the ankle joint with precision that ultrasound cannot reach. Osteochondral lesions, which are areas where cartilage and the underlying bone have separated or deteriorated, are among the most commonly missed injuries after ankle sprains. These lesions cause persistent deep joint pain and will not heal correctly without targeted intervention, so identifying them early through MRI prevents years of chronic symptoms and progressive joint damage.
MRI is the only imaging tool that simultaneously evaluates bone marrow, cartilage, tendons, ligaments, and nerves in a single study without using any radiation.
When your doctor will order an MRI
Your podiatrist will typically order an MRI when your symptoms have continued beyond the expected healing window despite appropriate initial treatment, or when X-ray and ultrasound results do not fully explain the severity of your pain. It’s also the first choice when nerve compression is suspected, since MRI can identify masses, scar tissue, or anatomical abnormalities pressing on the tibial nerve or its branches in the tarsal tunnel area.
One practical consideration is that metal implants from prior foot or ankle surgery may limit the quality of MRI images or disqualify you from the scan entirely, depending on the type of hardware. In those situations, your doctor will discuss whether a CT scan or ultrasound covers your diagnostic needs adequately. For patients without implant concerns, MRI delivers a comprehensive view that supports confident, well-informed treatment decisions from surgical planning to targeted physical therapy protocols.
CT for fractures and complex bone anatomy
Computed tomography, commonly called a CT scan, uses X-ray beams taken from multiple angles to reconstruct detailed three-dimensional images of bone. Where a standard X-ray gives you a flat, two-dimensional picture, CT stacks hundreds of cross-sectional slices into a complete model of your foot and ankle. That depth of detail makes it the preferred tool whenever fracture complexity, bone alignment, or surgical planning requires a level of precision that a single-angle X-ray cannot deliver.
What CT shows that X-ray misses
Standard X-rays can identify most obvious fractures, but small fracture lines that run parallel to the X-ray beam often disappear entirely on a flat image. CT eliminates that problem by imaging the same bone from every direction simultaneously. A calcaneus fracture, for example, may show on X-ray as a general collapse of the heel bone, while CT reveals exactly how many separate bone fragments exist, where they’ve displaced to, and how the subtalar joint surface has been affected. That detail directly determines whether your surgeon operates and, if so, which approach to use.
Tarsal coalition, a condition where two bones in the midfoot or hindfoot fuse together abnormally, is another diagnosis that CT identifies with far greater accuracy than any other imaging modality. The coalition can be fibrous, cartilaginous, or fully bony, and CT distinguishes between all three. Knowing the type and extent of the connection guides whether your podiatrist recommends a conservative approach, resection of the coalition, or a joint fusion procedure.
CT delivers the most precise three-dimensional picture of bone structure available, making it essential for any condition where fracture pattern or bone geometry determines the treatment plan.
When your doctor will order a CT scan
Your clinician will typically request a CT scan after an X-ray confirms a fracture but doesn’t show enough detail to plan the next step. Lisfranc injuries, which involve the joints between your midfoot and forefoot bones, are a strong example. These injuries frequently appear subtle or even normal on standard X-ray, but CT imaging reveals the subtle diastasis and bone chip fractures that confirm the diagnosis and indicate whether surgical stabilization is necessary.
Foot and ankle imaging with CT is also the standard of care before complex reconstructive surgery, joint replacement, or correction of severe deformity. Your surgical team uses the three-dimensional reconstruction to measure bone angles, evaluate joint involvement, and design the approach before you enter the operating room. That preparation reduces surgical time and improves the precision of every step in your procedure.
Contrast and nuclear medicine imaging when needed
Most foot and ankle problems resolve through standard X-ray, MRI, ultrasound, or CT. But when those studies return unclear results or when your clinician suspects bone infection, tumor activity, or complex vascular involvement, additional imaging techniques step in to fill the diagnostic gap. These advanced options are used selectively, but they can be decisive when standard imaging leaves important questions unanswered.
Contrast-enhanced MRI and CT
Your doctor may order contrast material, typically a gadolinium-based injection given through a vein, before or during an MRI when soft tissue infection, inflammatory arthritis, or a suspicious mass requires sharper differentiation between tissue types. Contrast highlights areas where blood supply is elevated, which occurs in infected tissue, actively inflamed joints, and certain tumors. Foot and ankle imaging with contrast-enhanced MRI is particularly valuable when osteomyelitis, a deep bone infection, needs to be confirmed or ruled out in a diabetic patient with a non-healing wound.
CT angiography uses iodine-based contrast injected intravenously to map the blood vessels supplying your foot and ankle. When you have peripheral artery disease or a wound that isn’t healing despite treatment, CT angiography shows your surgeon exactly which vessels are patent, narrowed, or blocked. That vascular map directly influences decisions about revascularization procedures, amputation risk, and the likelihood of wound healing with conservative care.
Contrast imaging adds a layer of diagnostic precision that standard scans cannot match when infection, vascular disease, or soft tissue masses are part of the clinical picture.
Bone scan and nuclear medicine options
A bone scan, also called a three-phase nuclear bone scan, uses a small amount of radioactive tracer injected into your bloodstream to highlight areas of abnormal bone activity. The tracer accumulates in regions where bone cells are working harder than normal, such as in stress fractures, infections, and metastatic disease. Your clinician may recommend a bone scan when symptoms strongly suggest a stress fracture but MRI is not available or is contraindicated due to metal implants.
White blood cell scans take nuclear imaging a step further by tagging your own immune cells with a tracer and reimaging after several hours. Tagged cells concentrate in areas of active infection, making this study one of the most accurate tools available for diagnosing osteomyelitis in complex cases where MRI findings remain ambiguous. While these nuclear medicine studies involve low-dose radiation and require multiple imaging sessions over the course of a day, they provide functional information about bone and tissue activity that no anatomical scan can replicate.
Getting ready, safety, and understanding results
Knowing what to expect before, during, and after foot and ankle imaging makes the entire process smoother and helps you get the most from your appointment. Each imaging modality has its own preparation steps, safety profile, and result timeline, so understanding the basics ahead of time removes uncertainty and lets you focus on getting an accurate diagnosis.
How to prepare for each type of scan
X-ray and ultrasound require almost no advance preparation. You can eat, drink, and take your regular medications without any restriction before either study. Wear or bring comfortable clothing that allows your lower leg and foot to be uncovered easily, and remove any jewelry or metal accessories from your ankle before you arrive.
MRI preparation involves a few more steps, particularly if you have metal implants, a pacemaker, or any history of working with metal fragments. Your imaging center will ask you to complete a safety screening form before you enter the scan room. CT scans are similarly straightforward unless contrast dye is being used, in which case your provider may ask you to fast for a few hours beforehand and will check your kidney function to confirm your body can clear the contrast safely.
Completing your safety screening form honestly and thoroughly is one of the most important steps you take before any imaging study.
Understanding radiation and scan safety
Standard foot and ankle X-rays and CT scans use ionizing radiation at very low doses, and the diagnostic benefit in these studies far outweighs the minimal risk for most patients. Your imaging team follows established protocols to limit your exposure to only what’s necessary for a clear, diagnostic-quality image. Pregnant patients should always inform the technician before any scan so that appropriate shielding or alternative imaging can be arranged.
MRI and ultrasound use no ionizing radiation at all, making them particularly suitable for repeat imaging or for patients who need ongoing monitoring. Ultrasound is safe across all age groups and medical conditions without restriction.
Making sense of your results
Your podiatrist reviews imaging results in the context of your full clinical picture, not in isolation. A finding that looks significant on a scan may be a normal variation for your anatomy, while a subtle change on one image might explain every symptom you’ve described. Ask your provider to walk you through the images directly so you understand exactly what was found, what it means for your condition, and how it shapes your treatment plan going forward. Written reports are useful references, but a direct conversation with your clinician gives you the clarity you need to move forward with confidence.
What to do next
Foot and ankle imaging gives your care team the precise diagnostic information they need to move your treatment in the right direction from day one. The right scan at the right time shortens your path to recovery, whether you’re dealing with a fresh ankle sprain, chronic heel pain, or a complex condition that hasn’t responded to previous care. Understanding which imaging tool fits your situation is the first step, and your podiatrist handles that decision based on your specific symptoms and history.
You don’t have to figure out what comes next on your own. The specialists at Achilles Foot and Ankle Center are ready to evaluate your foot or ankle concern, order the appropriate imaging, and build a treatment plan around what the results show. Same-day appointments are available across our Central Virginia locations, so you can get answers quickly without a long wait. Schedule your same-day appointment and take the first step toward lasting relief.