Your foot is swollen, warm, and red, but you don’t remember injuring it. If you have diabetes or nerve damage, this scenario should raise immediate concern. Understanding what is Charcot foot could mean the difference between early intervention and permanent disability.
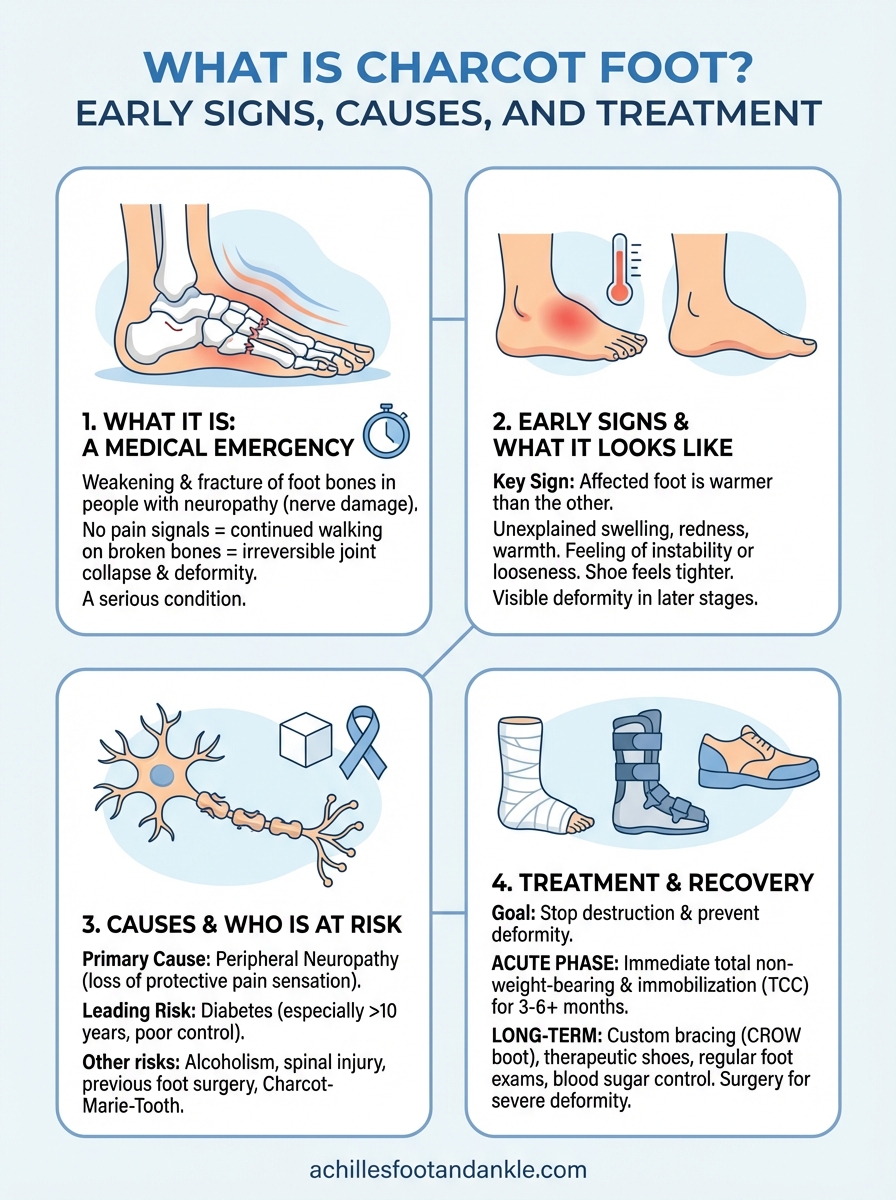
Charcot foot (also called Charcot arthropathy) is a serious condition that weakens the bones in your foot, often leading to fractures, joint collapse, and severe deformity. It primarily affects people with peripheral neuropathy, which is why diabetic patients face the highest risk. Because numbness masks the pain that would normally signal a problem, many people continue walking on damaged bones without realizing the damage they’re causing.
At Achilles Foot and Ankle Center, our diabetic foot care and limb salvage programs treat patients across Central Virginia who are dealing with this condition. In this guide, we’ll explain how Charcot foot develops, the early warning signs you shouldn’t ignore, and the treatment approaches that can help preserve your mobility and prevent amputation.
Why Charcot foot is a medical emergency
Understanding what is Charcot foot becomes urgent when you realize how quickly this condition progresses without immediate treatment. The weakened bones in your foot begin to fracture under normal weight-bearing activities, and because neuropathy blocks pain signals, you continue walking on broken bones. Each step drives those fractures deeper, crushing healthy bone structure and causing irreversible joint collapse that can happen within weeks or months.
The progressive nature of bone damage
Charcot foot develops in distinct stages, and the acute phase (when your foot first shows redness, swelling, and warmth) represents a critical window for intervention. During this stage, your bones are actively breaking down, and the inflammatory response creates a destructive cycle. Your body attempts to heal the microfractures, but continued pressure from walking prevents proper healing and instead accelerates the destruction. Medical literature shows that patients who delay treatment during this acute phase face significantly higher rates of permanent deformity.
The acute inflammatory phase typically lasts 3 to 6 months, during which your foot literally reshapes itself under the stress of continued weight-bearing.
Why continued walking accelerates destruction
Your inability to feel pain removes the natural protective mechanism that would force you to stop walking. When healthy bones fracture, sharp pain immediately alerts you to the injury and limits your movement. In contrast, Charcot foot allows you to continue your daily activities while bones splinter and joints disintegrate beneath the surface. Each additional day of walking on the affected foot compounds the damage, shifting bones out of alignment and creating the characteristic "rocker-bottom" deformity where the arch completely collapses. This deformity develops when the midfoot bones fragment and settle, pushing the bottom of your foot outward and creating an unstable walking surface.
The risk of amputation and permanent complications
Untreated Charcot foot leads to severe complications that threaten your ability to walk and, ultimately, your limb itself. Bone deformities create pressure points that develop into chronic ulcers, especially on the collapsed arch or protruding bone surfaces. These ulcers frequently become infected because the compromised blood flow and nerve damage already present in diabetic patients prevent proper healing. Studies indicate that 15-20% of Charcot foot patients require amputation when the condition goes unrecognized or untreated.
Beyond amputation risk, you face permanent mobility loss even with successful limb salvage. Severe joint destruction requires extensive reconstructive surgery, prolonged immobilization, and months of rehabilitation. Some patients never regain their previous walking ability and require custom bracing or wheelchairs for life. The economic burden extends beyond medical costs to include lost work productivity, home modifications, and ongoing care needs. Seeking immediate evaluation when you notice unexplained swelling, redness, or warmth in your foot can prevent these devastating outcomes and preserve your independence.
Early signs and what Charcot foot looks like
Recognizing the early signs of Charcot foot requires attention to subtle changes that many diabetic patients dismiss as minor issues. Your foot may show noticeable warmth and redness without any obvious injury or infection, often appearing suddenly over several days. The affected foot typically feels warmer to the touch than your other foot, and you might notice swelling that persists throughout the day, even after rest. These symptoms appear because inflammation floods the area as bones begin breaking down internally.

The initial warning symptoms
The earliest indication often involves a difference in temperature between your feet, with the affected side feeling significantly warmer when you touch both simultaneously. You may experience a feeling of instability or looseness in your ankle or foot, as if the structure inside has shifted. Some patients report a vague sensation of discomfort or pressure, though true pain remains absent due to neuropathy blocking those signals. Your shoe might suddenly feel tighter on one side, indicating rapid swelling that develops as the bone destruction progresses.
Up to 75% of Charcot foot cases initially get misdiagnosed as simple sprains or infections because the symptoms seem too mild to indicate serious bone damage.
Visual changes you can observe
Looking at your foot reveals distinct redness that spreads across the arch and midfoot, resembling cellulitis but without the typical infection symptoms like fever or drainage. The swelling creates a puffy appearance that extends from the toes to the ankle, making the normal contours of your foot difficult to see. As the condition advances into later stages, you notice visible deformity where the arch collapses and the sole develops an abnormal bulge, creating what doctors call a rocker-bottom appearance. Your foot may appear twisted or shortened compared to your unaffected side, with bones protruding at unusual angles through the skin. These visible changes confirm that understanding what is Charcot foot matters critically, as they indicate extensive internal damage requiring immediate medical intervention before permanent deformity sets in.
What causes Charcot foot and who is at risk
Charcot foot develops when peripheral neuropathy eliminates your ability to feel pain, allowing repeated minor trauma to accumulate without your awareness. The condition requires two components: nerve damage that blocks protective pain signals and some triggering event like a minor sprain, fracture, or surgical procedure. Once trauma occurs, your body initiates an inflammatory response that weakens the surrounding bone structure, but because you can’t feel the injury, you continue walking and applying pressure that accelerates the bone destruction. This creates a destructive cycle where walking on weakened bones causes additional fractures and inflammation.
The role of neuropathy and diabetes
Diabetes represents the leading cause of Charcot foot, accounting for approximately 80% of all cases. High blood sugar levels over many years damage the nerves in your extremities through a process that gradually destroys the protective covering around nerve fibers. This diabetic neuropathy typically affects your feet first because the longest nerves in your body suffer the most damage. When you lose protective sensation, you can’t detect the microfractures and injuries that trigger Charcot foot development.
Your risk increases significantly if you’ve had diabetes for more than 10 years or if you already experience symptoms like numbness, tingling, or reduced temperature sensation in your feet. Poor blood sugar control accelerates nerve damage and creates the conditions where understanding what is Charcot foot becomes personally relevant.
Studies show that diabetic patients with neuropathy face a lifetime risk of developing Charcot foot between 0.1% and 0.9%, though this increases substantially with poor glucose management.
Other risk factors beyond diabetes
Several conditions beyond diabetes can cause the neuropathy necessary for Charcot foot to develop. Alcoholism damages peripheral nerves through both nutritional deficiencies and direct toxic effects on nerve tissue. Spinal cord injuries, particularly those affecting the lower spine, eliminate sensation in your feet and create vulnerability to this condition. Other neurological diseases like Charcot-Marie-Tooth disease or multiple sclerosis also compromise nerve function and increase your risk.
Recent foot or ankle surgery, particularly in patients with existing neuropathy, can trigger Charcot foot as the inflammatory response from surgery weakens surrounding bone. Your risk factors compound when multiple conditions coexist, making regular foot examinations critical if you have any form of peripheral nerve damage.
How doctors diagnose Charcot foot
Diagnosing Charcot foot requires a combination of clinical examination and imaging studies, as the condition often mimics other foot problems like infections or sprains. Your doctor begins by assessing your medical history and risk factors, particularly your diabetes status and presence of neuropathy. The diagnostic process focuses on identifying bone damage before it progresses to severe deformity, making early detection critical for preserving your foot structure.
Physical examination and clinical signs
During the physical exam, your podiatrist compares the temperature of both feet using either touch or an infrared thermometer, looking for a difference of more than 3-4 degrees Fahrenheit between sides. They assess swelling patterns, skin color changes, and any visible deformities that suggest bone collapse. Your doctor tests your sensation using monofilament testing or tuning forks to confirm neuropathy, as this nerve damage represents a necessary component of understanding what is Charcot foot and how it develops. They also check your foot’s stability by manipulating joints and feeling for abnormal movement that indicates ligament damage or bone fragmentation.
Imaging tests that reveal bone damage
X-rays provide the first-line imaging approach for diagnosing Charcot foot, revealing fractures, bone fragmentation, and joint dislocations that confirm the condition. However, early-stage disease may show minimal changes on standard X-rays, requiring more sensitive imaging methods. MRI scans detect bone edema and inflammation before fractures become visible, making them valuable for catching the acute phase when intervention is most effective. Your doctor may also order CT scans to evaluate the three-dimensional bone structure and plan surgical reconstruction if needed.

Early X-rays may appear normal despite active Charcot foot, which is why doctors rely heavily on clinical signs like warmth and swelling to make the initial diagnosis.
Blood tests help rule out infection by checking inflammatory markers and white blood cell counts, as the redness and swelling can resemble osteomyelitis. Your doctor may order serial X-rays taken weeks apart to track progression and confirm the diagnosis, as Charcot foot shows characteristic changes over time that distinguish it from other conditions affecting diabetic feet.
Treatment options and what recovery involves
Treatment for Charcot foot focuses on stopping the destruction process and preventing permanent deformity, which requires immediate intervention once your doctor confirms the diagnosis. The primary goal centers on immobilizing your affected foot completely to allow bones to stabilize and inflammation to subside. Your treatment plan varies based on the stage of Charcot foot you’re experiencing, with acute phase patients receiving aggressive non-surgical management while those with established deformities may require reconstructive surgery.
Immobilization as the foundation of treatment
Your doctor prescribes total non-weight-bearing status using crutches, a knee scooter, or wheelchair for the initial treatment period, which typically lasts 8 to 12 weeks. You wear a total contact cast (TCC) that protects your foot while distributing pressure evenly across the entire surface, preventing additional bone collapse. This cast requires changing every 1 to 2 weeks as swelling decreases, and your podiatrist monitors healing through serial X-rays and temperature measurements.
Most patients need at least 3 to 6 months of immobilization before the inflammatory process subsides enough to permit gradual weight-bearing activities.
After the acute phase resolves, you transition to custom-molded bracing like a CROW boot (Charcot Restraint Orthotic Walker) or ankle-foot orthosis that provides ongoing protection while allowing limited mobility. This bracing phase continues for several months or longer, depending on your bone healing progress.
Surgical intervention and reconstruction
Surgery becomes necessary when severe deformity creates pressure points that lead to ulcers or when your foot structure becomes too unstable for bracing alone. Reconstructive procedures involve realigning collapsed bones, removing prominent areas, and stabilizing joints with internal hardware like plates, screws, and external fixators. Your surgeon may perform bone fusion to create a stable platform for walking, though recovery requires 4 to 6 months of non-weight-bearing followed by gradual rehabilitation.
Long-term management and lifestyle adjustments
Understanding what is Charcot foot means recognizing that recovery extends beyond initial treatment into lifelong protective measures. You need custom therapeutic shoes with specialized insoles that redistribute pressure away from vulnerable areas. Regular foot examinations, strict blood sugar control, and immediate attention to any new swelling or warmth help prevent recurrence in your treated foot or development in your other foot.
Key takeaways
Understanding what is Charcot foot empowers you to recognize the warning signs before permanent deformity develops. This serious condition destroys bone structure in your foot when neuropathy blocks pain signals, allowing you to walk on fractures without realizing the damage. Warmth, swelling, and redness in your foot require immediate medical evaluation, particularly if you have diabetes or nerve damage. Early intervention through immobilization can preserve your foot structure and maintain your ability to walk independently, while delayed treatment often leads to severe complications including amputation. The key to successful outcomes lies in catching the acute inflammatory phase when bones first begin breaking down.
If you experience unexplained swelling or warmth in your foot, contact Achilles Foot and Ankle Center for evaluation. Our diabetic foot care specialists provide comprehensive assessment and treatment across Central Virginia, with same-day appointments available for urgent concerns. Protecting your mobility starts with recognizing the signs and seeking expert care before bone damage becomes irreversible.