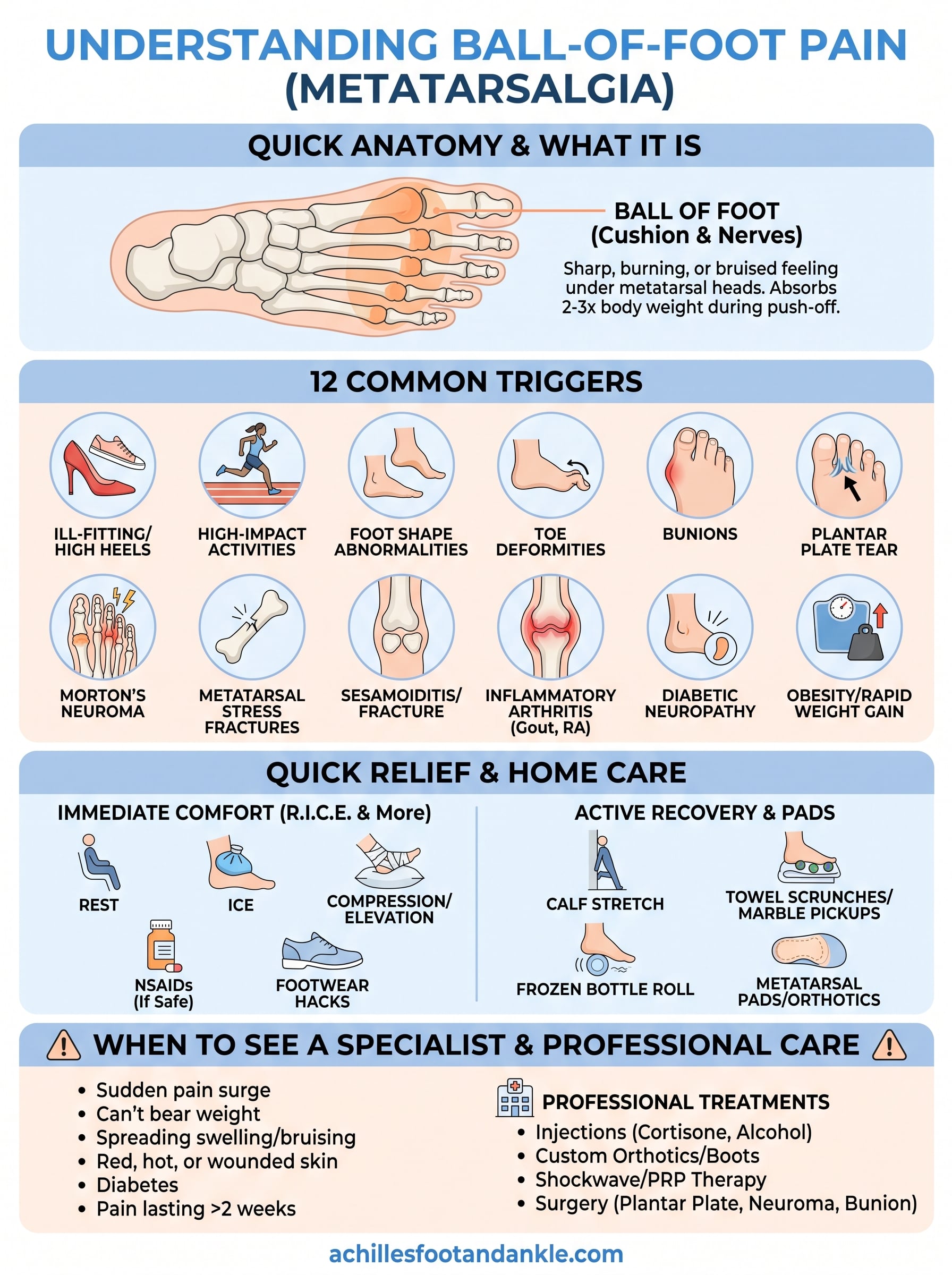
Ball-of-foot pain, often labeled metatarsalgia, is the sharp, burning, or bruised feeling lodged beneath the heads of your metatarsal bones. Whether it flares only during a morning run or pulses with every stride, that pinpoint ache can turn a short errand into a chore, and you want to know why.
This guide walks you through 12 frequent triggers, explains how to match your symptoms to likely causes, shows quick relief tactics you can start at home, and pinpoints the moments when professional care at Achilles Foot and Ankle Center becomes the smartest move. All information is for general education; it’s not a substitute for a personalized evaluation or treatment plan from a licensed podiatrist.
Quick Anatomy Refresher: Why the Ball of Your Foot Works So Hard
Where is the ball of your foot, exactly? It’s the padded, weight-bearing cushion on the sole of your foot, sitting between your arch and your toes, right where the five metatarsal heads line up like tiny door-knobs just behind your toe joints. Each head meets its matching toe bone at a metatarsophalangeal (MTP) joint, letting your toes hinge as you push off. Beneath this hardware sits the plantar fat pad, a springy gel-like cushion, and a bundle of interdigital nerves that weave between the metatarsals.
Every time you walk or sprint, the toe-off phase funnels two to three times your body weight through this postage-stamp-sized area. When you jump or pivot, the load spikes even higher. Add in the natural thinning of the fat pad with age, and those bones and nerves lose their built-in shock absorber, making the region extremely sensitive to even minor changes in pressure.
Key Takeaway
A small, nerve-rich area absorbing outsized forces means tweaks in shoes, weight, or anatomy can quickly translate into ball-of-foot pain.
12 Common Triggers of Ball of Foot Pain
Before you can tame the ache, you need to know what causes ball of foot pain in the first place. The list below covers the usual suspects, but remember that two, or even three, triggers often gang up together. For example, a runner with high arches who just switched to minimal shoes may check three boxes at once.
1. Ill-Fitting or High-Heeled Shoes
Narrow toe boxes and stiletto-style heels shove body weight toward the forefoot and cram the metatarsal heads together. Athletic cleats with stiff soles can do the same.
- Clue: Pain eases minutes after you kick the shoes off.
2. High-Impact Activities (Running, Court Sports, Dance)
Every hard landing multiplies forefoot load; ramping up mileage or practice hours too fast magnifies the stress. Rest days and shock-absorbing footwear are protective.
3. Foot Shape Abnormalities (High Arches, Flatfeet)
A high-arched (cavus) foot acts like a rigid lever, concentrating pressure under the first and fifth metatarsals. Excess pronation in flatfeet overloads the second metatarsal instead.
4. Toe Deformities: Hammertoes & Claw Toes
When toes bend downward permanently, they stop sharing push-off duties, passing the workload, and the pain, back to the metatarsal heads.
5. Bunions (Hallux Valgus)
As the big toe angles inward, it crowds the second toe and forces you to roll weight onto the adjacent metatarsal, a common metatarsalgia hotspot.
6. Plantar Plate Tear or Instability
A tiny ligament under the second toe rips or stretches, triggering sharp, pinpoint pain and sometimes causing the toe to drift sideways or skyward.
7. Morton’s Neuroma
Thickening of the interdigital nerve between the third and fourth metatarsals produces burning, tingling, or the feeling of a pebble in the shoe. Tight shoes make it scream.
8. Metatarsal Stress Fractures
Microscopic cracks from overuse present as localized swelling and night pain that improves with rest but returns when you walk barefoot.
9. Sesamoiditis & Sesamoid Fracture
The two sesame-seed-size bones under the big-toe joint become irritated, or break, after repeated push-offs or high-heel use. Pain spikes when you tiptoe.
10. Inflammatory Arthritides (Gout, RA)
Gout strikes suddenly with redness and searing pain, often at night. Rheumatoid arthritis causes chronic forefoot stiffness and morning soreness.
11. Diabetic Neuropathy & Fat-Pad Atrophy
Loss of protective sensation plus thinning fat pads raises plantar pressures and encourages callus formation, a double hit for people with long-standing diabetes.
12. Obesity & Rapid Weight Gain
Every extra pound equals roughly two to three additional pounds of force at toe-off. Sudden weight gain offers the foot no time to adapt.
Self-Check Table
| Symptom Pattern | Likely Cause(s) |
|---|---|
| Burning or pebble sensation between 3rd–4th toes | Morton’s neuroma |
| Sharp stab under 2nd toe, toe drifting | Plantar plate tear |
| Pain only in dress shoes or cleats | Ill-fitting/high-heeled shoes |
| Bruised feeling after mileage jump | Stress fracture, high-impact activity |
| Overnight onset with redness and swelling | Gout flare |
Use the table as a starting point, not a final diagnosis. When in doubt, book a professional evaluation.
Diagnosing the Culprit: What Happens at a Podiatry Visit
A proper work-up is equal parts detective work and high-tech imaging. Your podiatrist starts with an in-depth history, shoes, sports, job duties, medical conditions, then presses along each metatarsal head, performs a Mulder’s click test for neuroma, and checks toe stability with a plantar-plate “drawer” maneuver. Weight-bearing X-rays rule out fractures or joint misalignment; ultrasound can spot a swollen interdigital nerve, while MRI confirms hairline stress fractures or soft-tissue tears. Many clinics, including Achilles Foot and Ankle Center, add computerized pressure mapping to pinpoint overload zones and record slow-motion video of your gait so subtle compensation patterns don’t slip by.

Questions Your Doctor Will Ask
- When did the pain start, and has it changed?
- Which shoes make it better or worse?
- Recent mileage, training, or weight changes?
- Any numbing, tingling, or nighttime throbbing?
- Do you have diabetes, gout, or rheumatoid arthritis?
- Prior foot injuries or surgeries?
Simple At-Home Tests (Screening Only)
- Paper-Towel Dome: Roll a towel into a ½-inch log, stand with the painful spot directly over it. Pain that instantly eases points toward metatarsal overload treatable with a met-pad.
- Squeeze Test: Pinch the forefoot side-to-side; a “click” or electric jolt suggests Morton’s neuroma.
- Single-Toe Raise: Rise onto the affected toe; inability or pain under the 2nd toe hints at a plantar-plate tear.
These checks are clues, not confirmations, book an exam if any are positive or symptoms persist.
Fast Pain Relief You Can Start Today
Good news: many ball-of-foot flare-ups settle within days once you off-load the tissue and quiet inflammation. Try these quick, low-risk wins first.
- Rest: Swap running for cycling or plain old sitting for 24–48 hours.
- Ice: Place a pack (or bag of frozen peas) under the forefoot for 10 minutes, off for 10, repeat 3 times.
- Compression: Light elastic wrap around mid-foot keeps swelling in check, snug but never numb.
- Elevation: Prop the foot on pillows so it’s level with your heart whenever you’re parked on the couch.
- NSAIDs: Ibuprofen
200–400 mgevery 6–8 h, staying under1200 mg/dayunless your doctor okays more; skip if you have stomach, kidney, or blood-thinner issues. - Footwear hacks: Slip into a sneaker with a wide toe box and a heel drop < 1″; no barefoot walking on tile or concrete.
Targeted Exercises & Stretches
Keeping tissue mobile speeds recovery:
- Standing calf stretch: 30 s hold, 3 reps per side, twice daily.
- Towel scrunches: Sit, pull a towel with your toes for 1 min, rest 30 s, repeat 3 times.
- Marble pickups: 10 marbles, 2 sets.
- Frozen water-bottle roll under the ball of the foot for 5 min, up to 3×/day.
Pads, Inserts & Orthotics
A metatarsal pad placed just behind the sore spot (never on it) redistributes force; experiment with stick-on felt first. Store-bought cushioned insoles run $15–$40, while clinic-made custom orthotics cost $300–$500 but last years and correct underlying mechanics.
Does Massage Help?
Light cross-fiber massage or rolling a lacrosse ball under the forefoot for 60–90 seconds can boost blood flow and ease tight fascia. Stop if numbness, swelling, or a sharp “zing” appears, those signs mean see a pro instead of pushing harder.
Long-Term Fixes & Prevention Strategies
Quick fixes fade unless you address the overload. Build three habits: increase mileage gradually, rotate newer shoes, and keep body weight and foot muscles strong. Swap some road runs for cycling or pool workouts to spare the forefoot. Stick to the 10 % rule and retire running shoes every 300–500 miles. Even a modest 10-lb loss trims 20–30 lb of peak force felt at the metatarsal heads.
Footwear Buying Guide
- Firm heel counter
- Wide forefoot for toe splay
- Cushion or gentle rocker under met-heads
- Fit late day; thumb-width space at longest toe
Strength & Mobility Program
- Short-foot press: 3 × 10 holds daily
- Single-leg balance: 60 s each side
- Stair calf raises: 2 × 15
- Kneeling ankle dorsiflex stretch: 3 × 30 s
When It’s Time to Call in a Specialist
Most ball-of-foot twinges settle with rest and shoe tweaks, but certain warning signs call for expert eyes. Make the appointment if pain surges suddenly, you can’t put full weight on the foot, swelling or bruising spreads beyond the forefoot, or the skin looks red, hot, or wounded. Diabetics should be extra cautious, loss of sensation can mask serious injury. And if that nagging ache hangs on longer than two weeks despite diligent self-care, it’s time to bring in a podiatrist.
Professional Treatment Options
- Image-guided corticosteroid or alcohol injections to calm a Morton’s neuroma
- Custom orthotics or carbon-fiber plates to off-load tender metatarsals
- Cam-walker boots or bone stimulators for stress fractures that won’t heal
- Shockwave or platelet-rich plasma (PRP) therapy to jump-start stubborn soft-tissue repair
- Surgical procedures, plantar plate repair, neuroma excision, bunion correction, reserved for cases where conservative care fails
Your Next Steps
Most ball-of-foot pain boils down to three overlapping themes: mechanical overload, structural quirks, or systemic disease. Now that you know what causes ball of foot pain and how to spot the common patterns, keep a quick log of when symptoms spike, which shoes you had on, and what activities came before the ache. Swap in roomier, cushioned footwear, begin the gentle stretches and met-pad trick outlined above, and watch for steady improvement over the next week or two.
If the pain plateaus, worsens, or you notice red-flag signs, don’t tough it out, prompt evaluation prevents small problems from snowballing into fractures or nerve damage. Central Virginia readers can schedule a same-week visit with the team at Achilles Foot and Ankle Center for a customized game plan.