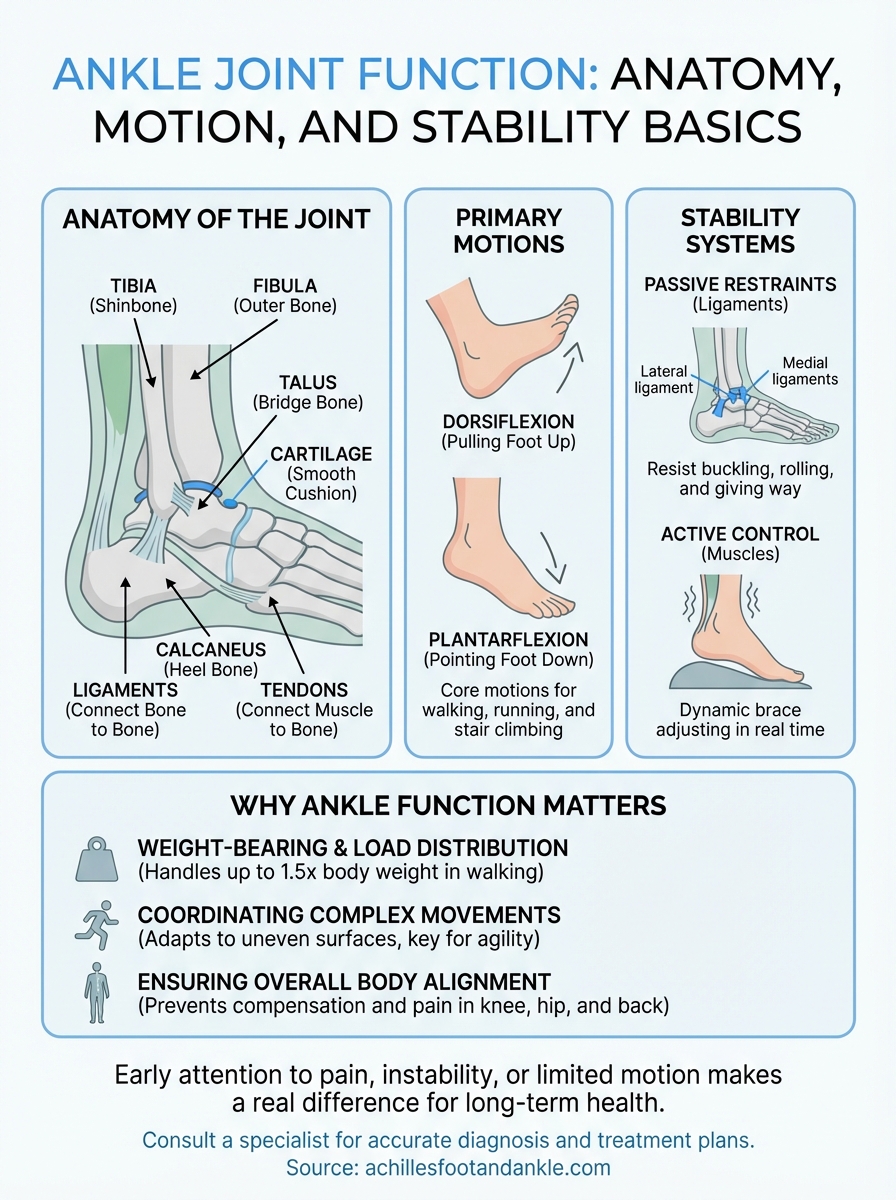
Your ankle does a remarkable amount of work every single day. It absorbs the shock of each step, adapts to uneven ground, and transfers force from your leg to your foot, all without you giving it a second thought. Understanding ankle joint function starts with recognizing just how much this joint handles: bearing your full body weight, coordinating complex movements, and keeping you stable whether you’re walking to your car or sprinting across a field.
The ankle allows two primary motions, dorsiflexion (pulling your foot up) and plantarflexion (pointing it down), but the full picture involves multiple bones, ligaments, and tendons working together in a tightly coordinated system. When any one of those structures is compromised by injury, disease, or wear, the effects ripple through your entire ability to move. That’s why a clear grasp of ankle anatomy and mechanics matters, especially if you’re dealing with pain or instability that won’t resolve on its own.
At Achilles Foot and Ankle Center, our specialists across Central Virginia diagnose and treat the full spectrum of ankle conditions, from chronic instability to post-surgical rehabilitation. This article breaks down the anatomy behind your ankle’s movement, explains how each structure contributes to stability and weight-bearing, and gives you the foundation to better understand what’s happening when something goes wrong, and what can be done about it.
Why ankle joint function matters
Your ankle is the bridge between your leg and the ground, and every step you take puts that bridge to the test. Most people only think about their ankles after something goes wrong, but understanding why ankle joint function is central to your overall movement can help you recognize problems before they become serious. The ankle doesn’t just flex and point. It coordinates load distribution, adapts to uneven surfaces, and plays a key role in keeping your entire lower body aligned.
The ankle as your body’s foundation
Each time your foot contacts the ground during a normal walking step, the force traveling through your ankle can reach one and a half times your body weight. When you run, that figure jumps to three or four times your body weight, depending on your pace and the surface beneath you. Your ankle handles these loads thousands of times per day, often without any conscious effort on your part.
This constant mechanical demand makes the ankle one of the most heavily stressed joints in the body. The bones, cartilage, tendons, and ligaments all absorb and redirect force at the same time. When any one of those structures is even slightly compromised, your body compensates by shifting load to other areas. That is how an untreated ankle problem can gradually affect your knee, hip, and lower back over time, turning what started as a local issue into a pattern of pain across your whole lower body.
Poor ankle mechanics rarely stay isolated. The compensation patterns they create often become the source of pain in joints well above the ankle.
What happens when ankle function breaks down
When ankle function declines, whether from an old sprain, arthritis, tendon damage, or nerve issues, the effects can appear in ways that feel unrelated at first. You might notice increased fatigue in your legs after short walks, or a tendency to roll your foot inward or outward when climbing stairs. Some people develop calluses or pressure sores in unusual spots because their foot is compensating for restricted ankle motion without them realizing it.
Reduced ankle mobility also overloads the Achilles tendon, the plantar fascia, and the smaller stabilizing muscles surrounding the joint. Over time, these structures become inflamed and painful, turning a mechanical problem into a daily obstacle. For people managing diabetes, that kind of abnormal pressure distribution raises the risk of ulcers and serious foot wounds that require advanced wound care intervention.
Why early attention makes a real difference
Catching ankle problems early gives you significantly more treatment options. A mild ligament strain addressed within the first few weeks often responds well to conservative measures such as targeted exercises, bracing, and physical therapy. Left unmanaged, the same sprain can lead to chronic instability, where the joint gives way repeatedly and cartilage damage accumulates with each episode.
The same principle applies to degenerative conditions like ankle arthritis. Early intervention can slow joint space loss, preserve motion, and delay or avoid the need for surgical reconstruction. Whether you are an athlete pushing through persistent discomfort or an older adult noticing changes in your balance, addressing ankle problems earlier consistently produces better long-term outcomes and keeps you doing the activities that matter to you.
Anatomy of the ankle joint in plain English
The ankle looks simple from the outside, but underneath the skin sits a precise assembly of bones, cartilage, tendons, and connective tissue. Getting familiar with the basic anatomy helps explain why ankle joint function depends on so many structures working together, and why damage to even one component can shift how the entire joint performs. You do not need a medical background to understand this, just a clear picture of the parts involved.
The three bones that form the joint
Three bones make up the ankle joint itself. The tibia, your shinbone, forms the inner and upper surface of the joint. The fibula runs alongside it and creates the bony bump you can feel on the outside of your ankle. The talus sits below both bones, acting as the bridge between your lower leg and your foot. Together, the lower ends of the tibia and fibula form a socket called the mortise, and the rounded top of the talus fits inside that socket like a peg in a groove.
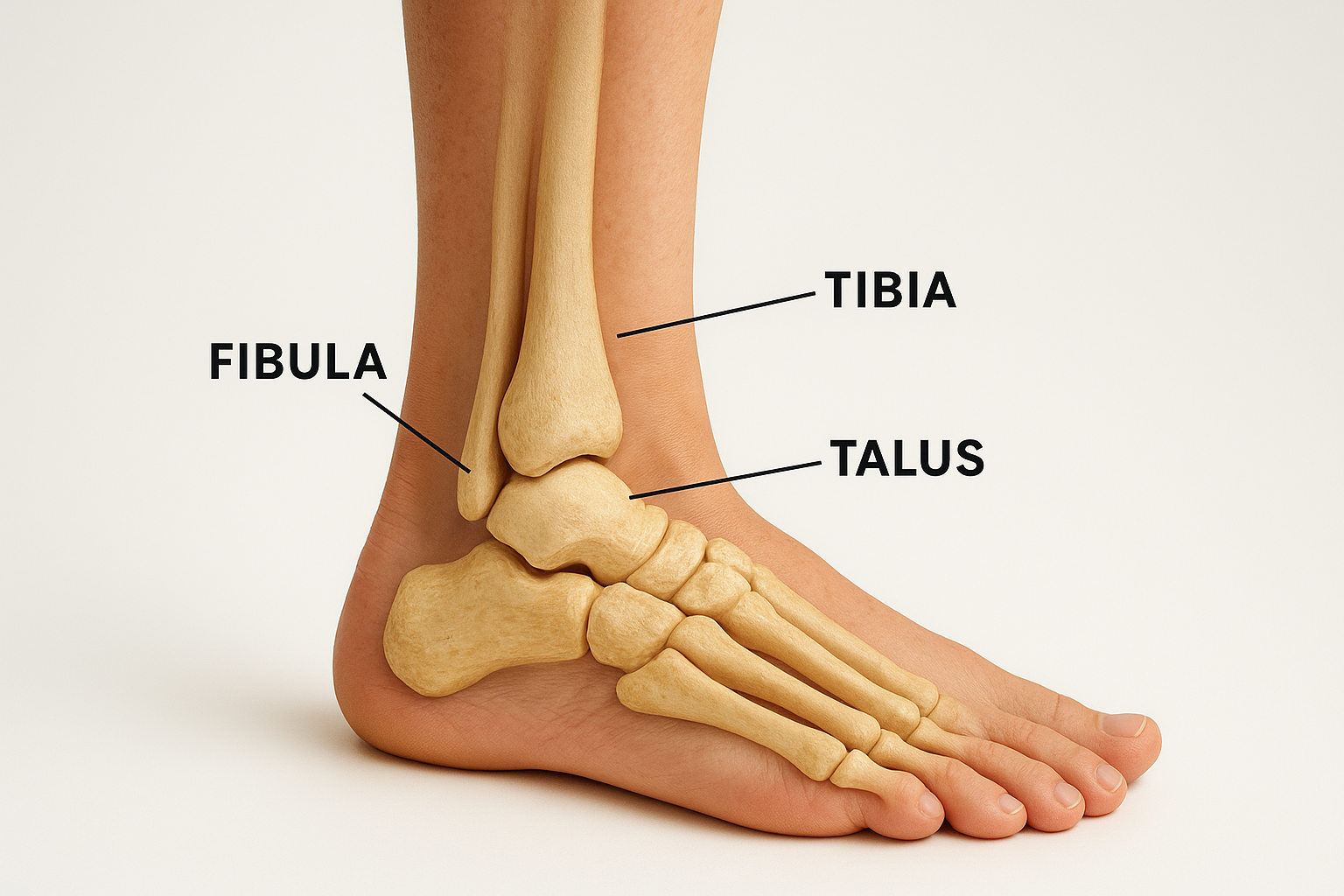
This mortise-and-peg arrangement gives the joint its core mechanical stability. The talus glides forward and backward within the socket, producing the up-and-down motion most people associate with ankle movement. A fourth bone worth knowing is the calcaneus, or heel bone, which sits directly below the talus and forms a separate structure called the subtalar joint. That joint handles the side-to-side tilting that lets you walk on uneven ground without constantly losing your footing.
The talus carries your entire body weight without a single muscle attaching directly to it, making the surrounding structures responsible for controlling every movement it makes.
Cartilage, tendons, and the surrounding soft tissue
A thin layer of smooth articular cartilage coats the surfaces of the tibia, fibula, and talus where they meet. This cartilage allows the bones to glide against each other with minimal friction and absorbs a portion of the load passing through the joint with each step. When cartilage breaks down from injury or arthritis, the joint loses that buffer, and bone-on-bone contact produces the grinding pain and stiffness that many patients describe as a deep ache that worsens with activity.
Multiple tendons cross the ankle in specific paths to control foot movement. The Achilles tendon connects your calf muscles to the back of the heel bone and drives the pushing-off motion in every step. Tendons along the front and sides of the ankle, including the tibialis anterior and peroneal tendons, control dorsiflexion and provide dynamic stabilization during walking and running. Inflammation or a partial tear in any of these tendons changes how load moves through the entire joint.
How the ankle moves: dorsiflexion and plantarflexion
The ankle produces two primary motions that drive nearly everything you do on your feet. Dorsiflexion brings the top of your foot toward your shin, while plantarflexion points your foot downward away from your leg. Together, these movements underpin the mechanics of walking, climbing stairs, and changing direction, making them the core expressions of healthy ankle joint function. Understanding both helps you recognize when something is limiting your range before that restriction starts causing problems elsewhere.

Dorsiflexion: pulling your foot up
Dorsiflexion happens every time your heel strikes the ground and your body rolls forward over your foot. The muscles along the front of your lower leg, especially the tibialis anterior, contract to lift the front of your foot and control how quickly it lowers after heel contact. Without adequate dorsiflexion, your foot slaps the ground awkwardly, and your body compensates by excessively rotating your hip or bending your knee, creating patterns that accumulate into overuse injuries over time.
Normal dorsiflexion range for most adults falls between 10 and 20 degrees past a neutral 90-degree position. If your ankle cannot reach that range, activities like squatting, walking uphill, or descending stairs become mechanically inefficient. A tight Achilles tendon is one of the most common reasons dorsiflexion becomes restricted, and it often goes unnoticed until the secondary effects start producing discomfort in the heel or knee. Consistent calf stretching and joint mobility work can preserve this range and reduce that downstream risk.
Limited dorsiflexion is one of the most frequently overlooked contributors to plantar fasciitis, Achilles tendinopathy, and knee pain in active patients.
Plantarflexion: pointing your foot down
Plantarflexion powers the push-off phase of every step you take. When your calf muscles, primarily the gastrocnemius and soleus, contract, they pull the heel upward through the Achilles tendon, driving your forefoot and toes into the ground and propelling your body forward. This motion also controls balance when you rise onto your toes and stabilizes your lower leg during activities that require rapid direction changes, such as pivoting or sprinting.
The range of plantarflexion typically spans 40 to 50 degrees in a healthy ankle. Weakness in the calf complex, partial Achilles tendon tears, or nerve damage affecting motor control can all reduce this range considerably. When plantarflexion is compromised, your stride length shortens and the muscles in your hip and thigh take on a larger share of the propulsive work, which increases fatigue and raises your injury risk during longer activities.
How the ankle stays stable: ligaments and muscles
Motion is only half the story of ankle joint function. Your ankle also needs to resist forces that would otherwise cause it to buckle, roll, or give way during everyday activity. That stability comes from two overlapping systems: passive ligament restraints that hold the bones in position, and active muscular control that adjusts in real time as your body moves. Both systems must be intact and communicating well for the joint to handle the demands placed on it safely.
The ligaments on each side of the ankle
Ligaments are tough bands of connective tissue that connect bone to bone, and the ankle relies on several of them to maintain alignment under load. On the outer side of the ankle, three ligaments form a group called the lateral ligament complex: the anterior talofibular ligament, the calcaneofibular ligament, and the posterior talofibular ligament. Of these, the anterior talofibular ligament is the most commonly injured, because it is the first structure stressed when your foot rolls inward, which is the mechanism behind most ankle sprains.
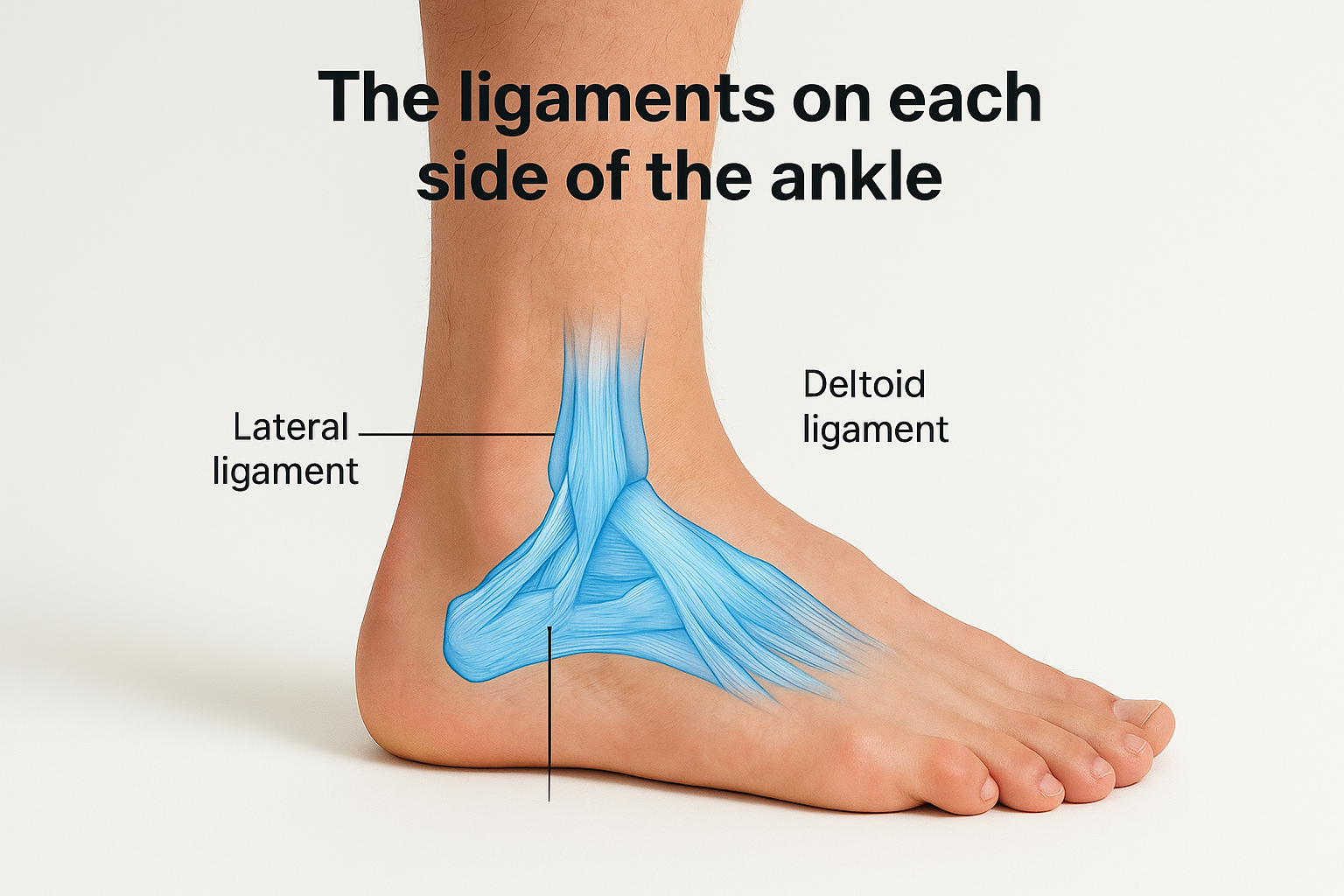
On the inner side, a broad, fan-shaped structure called the deltoid ligament resists outward rolling and provides medial stability. The deltoid is significantly stronger than the lateral complex, which explains why inward sprains are far more frequent than outward ones. These ligaments also carry sensory nerve endings that feed positional information back to your brain, so when a ligament tears, you do not just lose mechanical support, you also lose some of the joint’s proprioceptive signaling, which is the body’s awareness of where the ankle is in space.
Ligament damage that goes unrehabilitated often impairs proprioception more than it impairs structural stability, which is why balance retraining is a core part of ankle sprain recovery.
How muscles actively stabilize the joint
Your muscles act as a dynamic brace, firing rapidly to correct small shifts in joint position before they become larger problems. The peroneal muscles running along the outer lower leg are particularly important because they contract reflexively to prevent excessive inward rolling. When these muscles are weak or slow to respond, your ankle becomes vulnerable to repeated sprains even on relatively flat surfaces.
The muscles on the inner side of the lower leg, including the tibialis posterior, counterbalance the peroneals and also support the arch during weight-bearing. Targeted strengthening of both groups, combined with balance exercises that challenge the joint on unstable surfaces, restores the coordinated muscle activity that keeps your ankle protected during movement.
The ankle in walking, running, and balance
The ankle does not simply move, it sequences precisely timed actions that carry your body through space efficiently and safely. Every activity you perform on your feet, from a slow walk to a sprint to standing still on one leg, relies on coordinated ankle joint function to distribute load, generate propulsion, and maintain your center of gravity over your base of support.
How the ankle drives each walking step
Walking breaks into two phases: stance (when your foot is on the ground) and swing (when it is in the air). During stance, your ankle moves through a controlled sequence. At initial contact, your heel strikes the ground and dorsiflexion begins as your body rolls forward. Your ankle then reaches peak plantarflexion during push-off, where the calf muscles fire through the Achilles tendon and drive your forefoot into the ground, propelling you into your next stride.
Any restriction in that sequence forces compensations. If you cannot dorsiflex enough at mid-stance, your heel rises prematurely, your arch flattens under excess load, and your knee and hip rotate inward to make up for the lost motion. These patterns are subtle at first but compound quickly with repeated steps.
A single degree of lost dorsiflexion range can meaningfully alter load distribution across the foot and ankle over thousands of steps in a single day.
Running demands and ankle adaptation
Running multiplies the mechanical demands on every structure in the ankle. Ground contact time shortens, impact forces increase, and the ankle must absorb and redirect load faster than it does during walking. The peroneal muscles and tibialis posterior work together to stabilize the joint through each footstrike, while the Achilles tendon stores and releases elastic energy to improve running efficiency.
When these structures lack sufficient strength or flexibility, the ankle absorbs force poorly and transmits more stress to the plantar fascia, the shin, and the knee. Runners dealing with repetitive lower-leg pain often trace the problem back to a limitation in ankle mobility or single-leg calf strength.
Balance and the ankle’s proprioceptive role
Standing on one leg or navigating uneven terrain requires your ankle to make constant micro-adjustments in real time. The ligaments, joint capsule, and surrounding muscles all contain sensory receptors that feed positional data to your nervous system. Your brain processes that input and sends corrective signals back to the muscles within milliseconds, keeping you upright.
Previous ankle sprains reduce this sensory feedback, which explains why people with sprain history remain at higher risk of future injury even after the initial pain has resolved.
Common problems that affect ankle function
Several conditions can disrupt ankle joint function in ways that range from mildly inconvenient to severely limiting. Some develop after a single traumatic event, while others build gradually over months or years of accumulated stress. Knowing the most common culprits helps you connect symptoms to causes and take more targeted action when something feels wrong with your ankle.
Sprains and chronic instability
An ankle sprain occurs when the lateral ligaments stretch or tear beyond their normal range, most often during an inward rolling motion. Mild sprains involve minor ligament stretching, while severe ones include partial or complete tears that significantly compromise joint stability. The injury itself is common, but the real problem develops when sprains receive inadequate rehabilitation and the joint never fully regains its strength or proprioceptive signaling.
Chronic instability is the outcome of repeated, poorly managed sprains. Your ankle begins giving way on uneven surfaces, during direction changes, or even during routine walking. Each episode of giving way creates additional cartilage wear and ligament stress, accelerating joint degeneration over time. Balance retraining, strengthening of the peroneal muscles, and in persistent cases, ligament reconstruction are all options that address this pattern directly.
Untreated ankle instability progresses more predictably than most patients expect, making early rehabilitation one of the highest-return interventions available.
Arthritis and tendon damage
Ankle arthritis develops when the articular cartilage covering the joint surfaces breaks down, leaving bones with less cushioning against each other. Post-traumatic arthritis is the most frequent form in the ankle and typically follows a significant fracture or repeated instability. Symptoms include deep joint aching, morning stiffness, and swelling that worsens after prolonged activity and eases with rest.
Tendon problems cover a broad range of presentations. Achilles tendinopathy is one of the most common, involving degeneration of the tendon tissue from overuse or inadequate recovery between activity bouts. Peroneal tendon tears and tibialis posterior dysfunction are less familiar but equally disruptive, reducing the dynamic stability that muscles normally provide during movement. Both arthritis and tendon damage alter load distribution through the ankle, and both respond better to early treatment than to prolonged avoidance of the problem.
How to check ankle function at home
You don’t need specialized equipment or a clinical setting to get a basic picture of how your ankle is performing. A few straightforward self-assessments can reveal meaningful information about your range of motion, strength, and balance before you decide whether professional evaluation is warranted. These checks won’t replace a clinical examination, but they give you a starting point and help you communicate more clearly with a specialist if you do seek care.
Testing your range of motion
Dorsiflexion is one of the easiest aspects of ankle joint function to assess on your own. Stand facing a wall and place one foot about four inches from the base. Keep your heel flat on the floor and push your knee forward until it touches the wall. If your knee reaches the wall without your heel lifting, your dorsiflexion is likely within a functional range. Move your foot progressively farther from the wall to gauge how much range you actually have. Most adults should be able to manage this with the foot at least five inches from the wall.

For plantarflexion, sit on the floor with your leg extended and point your foot as far downward as it will go. Compare both sides directly. A noticeable difference between left and right often points to restricted mobility or tightness in the calf complex on the limited side, and that restriction alone can explain heel pain, arch discomfort, or knee strain that seems to have no obvious cause.
Even small side-to-side differences in range of motion deserve attention, especially if one side is consistently more restricted across multiple tests.
Checking balance and single-leg strength
Stand near a sturdy surface for safety and lift one foot off the ground. Time how long you can hold that position without touching anything for support. Most healthy adults under 60 can maintain single-leg balance for 30 seconds or more with reasonable steadiness. Struggling to reach 10 seconds points to a proprioceptive or strength deficit worth addressing. Test both sides and record any meaningful gap between them, since asymmetry is often more telling than the absolute number.
Next, try single-leg calf raises. Stand on one foot and rise onto your toes repeatedly at a controlled pace. You should complete at least 15 to 20 smooth repetitions without pain or fatigue cutting the set short. Fewer than 10 repetitions, discomfort during the movement, or visible compensatory leaning to finish the test all suggest calf strength or Achilles tendon issues that benefit from professional review.
How doctors evaluate ankle pain and instability
When you visit a specialist for ankle concerns, the evaluation goes well beyond pressing on the sore spot and sending you for an X-ray. A thorough clinical assessment looks at structural integrity, movement quality, and neuromuscular control to build a complete picture of how your ankle is actually performing. That layered approach is what makes it possible to identify the root cause rather than just the symptom.
Physical examination and movement testing
Your doctor starts by watching how you walk and bear weight before touching the ankle at all. Gait observation reveals compensatory patterns that rarely show up during a stationary exam, such as early heel rise, inward knee drift, or reduced push-off on one side. These movement clues point toward specific structures worth examining more closely.
The hands-on portion of the exam involves palpating each ligament, tendon, and bony landmark individually to localize tenderness. Specialized stress tests like the anterior drawer test and talar tilt test apply controlled force to the lateral ligaments to check whether they provide appropriate resistance. Single-leg stance and controlled reaching tasks assess proprioceptive function and dynamic stability, which is the part of ankle joint function that ligament damage most commonly disrupts. Weakness or hesitation during these tests helps your doctor distinguish between structural laxity and neuromuscular control deficits.
A clinical stress test tells you whether a ligament is mechanically intact; balance and strength testing tells you whether the nervous system around it is still working properly.
Imaging and diagnostic tools
X-rays are typically the first imaging step for any ankle complaint involving pain with weight-bearing, swelling after trauma, or suspected bone involvement. They confirm or rule out fractures, show joint space narrowing associated with arthritis, and reveal bony alignment problems that can drive chronic pain patterns.
When soft tissue damage is the concern, musculoskeletal ultrasound and MRI provide the detail that X-rays cannot. Ultrasound allows your doctor to examine tendons in real time, including during movement, which makes it particularly useful for identifying partial peroneal or Achilles tendon tears. MRI produces cross-sectional images of cartilage, ligaments, and bone marrow to detect pathology that does not appear on plain films. Your doctor selects the imaging approach based on clinical findings from the physical exam, not as a substitute for it, making that initial hands-on assessment the true foundation of an accurate diagnosis.
Next steps for a healthier ankle
Your ankle handles extraordinary mechanical demands every day, and every structure reviewed in this article plays a specific role in keeping that system running without pain or instability. When one component breaks down, the rest of the joint compensates, and those compensations rarely stay quiet for long. Understanding ankle joint function gives you the foundation to recognize early warning signs and act on them before they escalate into more serious problems.
If your self-assessments revealed limited range of motion, weak calf strength, or poor single-leg balance, those findings deserve professional attention rather than a wait-and-see approach. The specialists at Achilles Foot and Ankle Center evaluate the full picture, from bone alignment to neuromuscular control, and build treatment plans around your specific situation. Whether your concern is a nagging ache or recurring instability, getting accurate answers early consistently produces the best outcomes. Schedule an appointment today and take the first step toward keeping your ankle strong and functional.




