A sharp, stabbing pain in your heel, especially with those first steps in the morning, can stop you in your tracks. If you’ve been dealing with this kind of persistent discomfort, a heel spur may be the cause. Understanding heel spur diagnosis and treatment starts with knowing what you’re actually dealing with: a calcium deposit that forms on the underside of the heel bone, often developing over months and frequently linked to plantar fasciitis.
The good news is that most heel spurs respond well to non-surgical treatment. But getting the right diagnosis matters, because heel pain can stem from several different conditions, and each one calls for a different approach. An X-ray might reveal a spur you didn’t know you had, or rule one out entirely.
At Achilles Foot and Ankle Center, our podiatrists diagnose and treat heel spurs across thirteen locations in Central Virginia, using everything from custom orthotics and physical therapy to advanced imaging and surgical options when conservative care isn’t enough. This article walks you through how heel spurs are identified, what treatments are available, and when it’s time to consider surgery.
Why heel spurs happen and who gets them
Heel spurs don’t appear overnight. Your body deposits calcium on the heel bone (the calcaneus) in response to repeated stress and tension on the surrounding soft tissue. Over months, those deposits accumulate and harden into a bony protrusion that can reach up to half an inch in length. The process is gradual, and many people carry a heel spur for years before experiencing any pain at all.
How calcium builds up on the heel bone
The plantar fascia is a thick band of connective tissue that runs along the bottom of your foot, connecting your heel bone to your toes. When this tissue pulls repeatedly on the heel bone, your body responds by trying to repair the stress point. Calcium deposits accumulate where the plantar fascia attaches to the calcaneus, and over time they create the hook-shaped protrusion that shows up clearly on an X-ray.
This same mechanism can affect the Achilles tendon, which attaches to the back of the heel. A posterior heel spur forms when the Achilles tendon applies repeated strain on the calcaneus at its attachment site. Both types follow the same basic biology: consistent mechanical tension triggers calcium accumulation at the point where tissue meets bone, and the body keeps depositing more as long as the stress continues.
Heel spurs are a structural response to repeated stress, not a sign of disease or infection.
What activities and conditions trigger heel spurs
High-impact repetitive activity is one of the most direct triggers. Running long distances on hard surfaces, standing for hours on concrete, or jumping regularly in sports like basketball puts consistent strain on the plantar fascia and Achilles tendon. When your foot absorbs that load day after day without adequate recovery, the tissue repeatedly tugs on the heel bone and calcium starts to build.
Your footwear choices also play a significant role. Shoes with poor arch support, worn-out soles, or an improper fit fail to distribute pressure evenly across the foot. This concentrates stress on the heel, speeding up the tissue strain that leads to calcium deposits. Both flat-soled shoes and high heels shift load onto structures that aren’t designed to handle it over the long term.
Who is most likely to develop a heel spur
Certain groups face a higher statistical risk than others. Runners, especially those who increase their mileage too quickly, are among the most common patients. Workers who spend most of their shift on their feet, including nurses, teachers, warehouse and retail staff, also show up frequently in podiatry clinics with heel pain.
Excess body weight increases the load placed on the heel with every step, which accelerates wear on the plantar fascia and surrounding soft tissue. Age is another factor: the fat pad that cushions the heel thins naturally over time, leaving less protection between bone and ground. People over 40 are more likely to develop both plantar fasciitis and heel spurs as a result.
Certain structural foot characteristics raise your risk as well. Flat feet (overpronation) cause the arch to collapse inward with each step, placing extra tension on the plantar fascia. High arches create the opposite problem, reducing shock absorption and concentrating impact at the heel. Both conditions benefit from a proper heel spur diagnosis and treatment plan that addresses the underlying foot mechanics rather than the calcium deposit alone.
Symptoms and other causes of heel pain
Heel pain sounds straightforward, but the sensation you experience depends on what’s actually causing it. A heel spur can exist without producing any pain at all, while someone else with an identical spur on imaging can barely walk in the morning. Your symptoms tell the story, and paying close attention to when and where the pain occurs gives your doctor critical information during the diagnostic process.
What a heel spur feels like
Most people with a heel spur describe a sharp, knife-like pain on the underside of the heel when they stand up after sleeping or sitting for a long period. This first-step pain is the most consistent complaint, and it often eases slightly after you’ve been moving for a few minutes. The relief doesn’t mean the problem is gone; your soft tissue simply warms up and the immediate tension on the plantar fascia decreases.
Throughout the day, the pain can return after extended periods of standing or physical activity. Some patients describe it as a dull ache, while others feel a burning sensation that radiates toward the arch. Pressing firmly on the bottom of the heel often reproduces the pain directly, which is useful information during a physical exam as part of heel spur diagnosis and treatment.
If the pain is worst with your first few steps in the morning and improves slightly after walking, plantar fasciitis or a heel spur is the most likely explanation.
Other conditions that cause heel pain
Not every painful heel contains a spur, and several conditions produce nearly identical symptoms that require a different treatment approach. Plantar fasciitis is the most common culprit, caused by inflammation in the fascia itself rather than a bony deposit. In fact, many patients have plantar fasciitis without a spur, and many have a spur without significant fascia inflammation.
Stress fractures in the heel bone can also generate localized heel pain, particularly in runners or anyone who recently increased their training volume. Achilles tendinitis causes pain at the back of the heel rather than the bottom, while tarsal tunnel syndrome produces tingling and burning from nerve compression. Bursitis, an inflammation of the fluid-filled sacs near the heel, creates deep, pressure-sensitive pain that mimics a spur closely enough to require imaging to distinguish. Getting an accurate diagnosis rules out these alternatives before you commit to a specific treatment plan.
How doctors diagnose a heel spur
Getting a clear diagnosis is the foundation of any effective heel spur diagnosis and treatment plan. A podiatrist will use a combination of hands-on physical assessment and imaging to confirm whether a spur is present, determine its size and location, and identify any co-existing conditions like plantar fasciitis or bursitis that might be driving your pain.
The physical examination
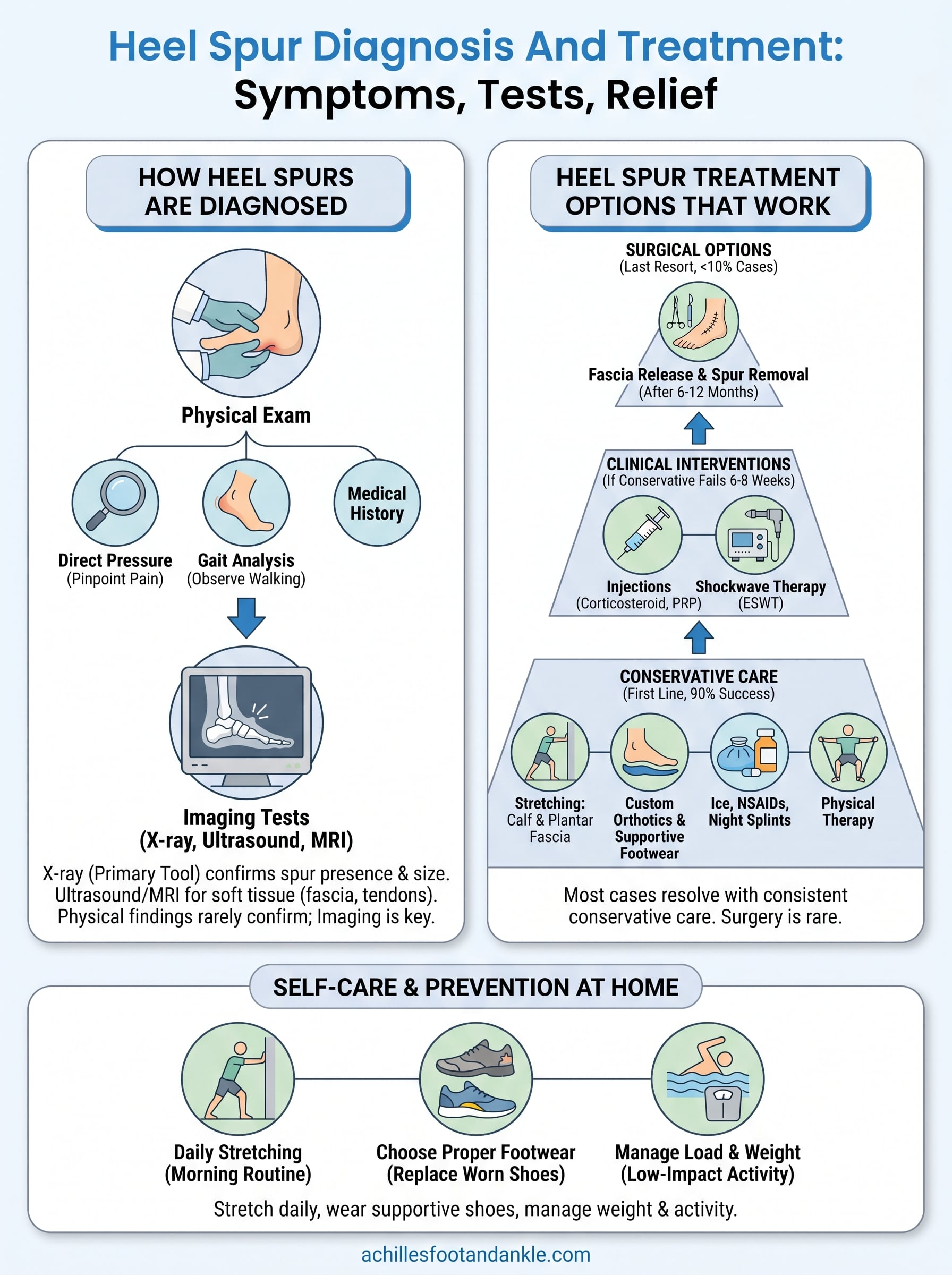
Your doctor starts by reviewing your medical history, activity level, and footwear habits before touching your foot. This background information narrows down the likely causes before the physical exam begins. Your podiatrist will then apply direct pressure to specific points on the heel to map where the pain originates. Pain concentrated at the bottom of the heel near the arch attachment point suggests plantar fascia involvement, while tenderness at the back of the heel points toward the Achilles tendon or a posterior spur.
Your podiatrist will also observe how you walk and how your foot makes contact with the floor. Overpronation, flat arches, or high arches all show up clearly in your gait and help explain why the spur developed in the first place. Range of motion tests assess how well your ankle and toe joints flex, since limited dorsiflexion (your ability to pull your toes upward) is a common finding in patients with plantar fascia tightness.
Physical exam findings alone rarely confirm a heel spur with certainty, which is why imaging is almost always the next step.
Imaging tests your doctor will order
An X-ray is the primary tool for confirming a heel spur. Calcium deposits show up clearly on standard weight-bearing X-rays, and the image gives your doctor exact measurements of the spur’s size and the direction it protrudes. Weight-bearing X-rays are particularly useful because they capture how your foot distributes load under real conditions, rather than in a non-loaded position that might underrepresent structural stress.

When soft tissue involvement needs closer evaluation, your doctor may order diagnostic ultrasound or an MRI. Ultrasound allows your podiatrist to assess plantar fascia thickness and detect tears or inflammation in real time, directly in the office. An MRI provides detailed cross-sectional images of both bone and soft tissue, which is especially useful when a stress fracture or nerve-related condition needs to be ruled out. Together, these tools give your care team a complete picture so that your treatment targets the actual source of your pain rather than a secondary finding.
Heel spur treatment options that work
Once your heel spur diagnosis and treatment plan is confirmed through imaging and physical exam, your podiatrist builds a treatment approach that starts with the least invasive options. Most patients never need surgery. Conservative care resolves symptoms in roughly 90 percent of cases when followed consistently over several months.
Conservative treatments: the first line of care
Your doctor will almost always begin with a combination of targeted stretching, activity modification, and supportive footwear. Calf and plantar fascia stretches reduce the tension that originally drove calcium buildup, and doing them consistently before your first steps in the morning makes a measurable difference. Custom orthotics go a step further by correcting the underlying biomechanical issues, such as overpronation or high arches, that continue to stress the heel.

Over-the-counter anti-inflammatory medications like ibuprofen or naproxen can reduce swelling and manage pain during flare-ups. Night splints hold your foot in a dorsiflexed position while you sleep, keeping the plantar fascia gently stretched so it doesn’t tighten overnight. Physical therapy adds structured exercises that build strength in the foot and lower leg, addressing muscular imbalances that standard stretching alone won’t fix.
Consistent stretching and custom orthotics, not rest alone, drive long-term improvement in most heel spur cases.
Clinical interventions when conservative care falls short
If six to eight weeks of conservative care hasn’t brought meaningful relief, your podiatrist has several clinical tools available. Corticosteroid injections deliver concentrated anti-inflammatory medication directly to the site of pain, providing faster relief than oral medications. These injections are typically guided by ultrasound to confirm precise placement and reduce the risk of soft tissue damage.
Extracorporeal shockwave therapy (ESWT) is a non-surgical option that uses acoustic wave energy to stimulate healing in chronic soft tissue injuries. Your podiatrist may also recommend platelet-rich plasma (PRP) injections, which concentrate growth factors from your own blood to accelerate tissue repair at the plantar fascia attachment site.
Surgery for heel spurs
Surgical treatment is reserved for a small percentage of patients who don’t respond after six to twelve months of documented conservative care. The procedure typically involves releasing part of the plantar fascia and removing the spur from the heel bone. Your surgeon will discuss the specific technique based on your imaging results and the location of the spur.
Recovery requires structured rehabilitation and gradual return to activity. Most patients return to full function within a few months when they follow their post-operative care plan closely.
Self-care and prevention at home
What you do between appointments has a direct impact on how quickly your heel heals and whether the problem returns. Consistent daily habits reduce the mechanical stress that drives both heel spur formation and the inflammation that makes existing spurs painful. A complete heel spur diagnosis and treatment plan always includes a home care component that you can start right away.
Build a daily stretching routine
The single most effective thing you can do at home is stretch your calf muscles and plantar fascia before putting weight on your foot each morning. Tight calf muscles limit ankle mobility, which forces your plantar fascia to absorb more load with every step. A simple calf stretch against a wall, held for 30 seconds on each side, reduces that tension significantly when done consistently.
The plantar fascia stretch is equally important. Pull your toes back toward your shin while seated, hold for 10 seconds, and repeat several times before your first steps of the day. Doing this before you stand up gives the tissue a chance to lengthen gradually rather than snapping tight under your full body weight. A towel or resistance band works well if reaching your foot is difficult.
Stretching for two to three minutes before getting out of bed each morning is the lowest-effort, highest-impact habit you can build for heel health.
Choose footwear that supports your foot mechanics
Your shoes either help your heel or hurt it every single day. Replace worn-out footwear regularly, particularly running shoes, which lose their shock absorption well before the upper shows obvious wear. Look for shoes with firm arch support, cushioned heel cups, and a slight heel lift rather than completely flat soles.
Avoid walking barefoot on hard floors, especially first thing in the morning. Tile and hardwood surfaces concentrate impact directly on an already-irritated heel. A supportive sandal or slipper kept beside the bed gives your plantar fascia the structure it needs before your muscles are warmed up.
Manage load and body weight over time
Reducing the total load your heel absorbs each day accelerates recovery and lowers your long-term risk. Swapping high-impact activities like running for lower-impact options such as swimming or cycling during flare-ups keeps you active without aggravating the tissue. Even small reductions in excess body weight measurably decrease the force your heel handles with every step, making consistent weight management a practical prevention strategy rather than just general health advice.
Get help for heel pain
Heel pain rarely improves on its own when the underlying cause goes unaddressed. Whether you’ve been dealing with sharp morning pain for weeks or a dull ache that flares up after activity, the right heel spur diagnosis and treatment plan can stop the cycle before it gets worse. Custom orthotics, targeted stretching, and clinical interventions like shockwave therapy or corticosteroid injections work best when they’re based on an accurate diagnosis, not guesswork.
At Achilles Foot and Ankle Center, our podiatrists serve patients across thirteen locations in Central Virginia and offer same-day appointments for urgent heel pain. You don’t need to keep working around the discomfort or waiting to see if it goes away. A physical exam and weight-bearing X-ray can confirm exactly what’s driving your pain and give you a clear path forward. Schedule your heel pain appointment today and get answers from a specialist who treats this every day.